When your child is diagnosed with autism spectrum disorder (ASD), one of the first questions that comes to mind is: Which will be better, home-based treatment vs. specialised autism center?
This decision shapes your child’s daily routine, learning environment, and long-term development. Therefore, it is vital to understand the real differences between the two options.
In this guide, we explore the difference between home-based treatment and specialised autism center in detail. We compare learning settings, therapy effectiveness, and family involvement.
Understanding Autism Therapy Options
Autism therapy focuses on improving communication, behaviour, independence, and social interaction. The most common approach is Applied Behaviour Analysis (ABA). However, ABA can be delivered in two main ways:
1. Home-based therapy
2. Centre-based therapy
This leads to a frequent debate: Home-based treatment vs. Specialised Autism Center.
There is no universal answer. Every child is unique. However, understanding the strengths and limitations of each model helps you choose wisely.
What Is Home-Based Autism Therapy?
Home-based therapy means that trained therapists visit your home and work with your child in familiar surroundings.
Key Benefits of Home-Based Therapy
Your child stays in a familiar environment
Therapy fits naturally into daily routines
Parents participate directly
Skills transfer easily to real-life situations
Limitations of Home-Based Therapy
However, home therapy also has challenges:
Fewer chances for peer interaction
Limited access to specialised equipment
Distractions at home can reduce focus
Progress depends heavily on parent involvement
So, while home therapy feels comfortable, it may not offer enough structure for all children.
The debate around Home-based treatment vs. Specialised Autism Center will continue. However, informed parents make confident decisions.
Home therapy offers familiarity and flexibility. Centre therapy offers structure and social exposure.
At India Autism Center, our goal is simple: To help every child reach their fullest potential.
If you are unsure about choosing Home-based vs. Center-based therapy, professional guidance can make all the difference.
Frequently Asked Questions (FAQs)
What is the difference between home-based treatment and a specialised autism center?
Home-based treatment happens in the child’s home with parent involvement, while a specialised autism center offers structured therapy, peer interaction, and professional facilities.
Is home-based ABA therapy better than centre-based ABA therapy?
Home-based ABA therapy is helpful for comfort and daily life skills, but center-based ABA therapy provides stronger structure and social learning. The best choice depends on your child’s needs.
How do I choose between home-based and center-based ABA therapy?
Choosing home-based vs. center-based ABA therapy depends on your child’s age, behaviour, sensory needs, family involvement, and access to specialised services.
Can home-based and center-based ABA therapy be combined?
Yes. Many families use a blended approach where skills are taught at a specialised autism center and practised through home-based therapy for better long-term outcomes.
For expert insights, support services, and inclusive learning initiatives, visit the India Autism Center.
It is a known fact that for children with Autism Spectrum Disorder, the world can feel overwhelming, whether it is loud noises or flashy lights. Parents often search for therapies that don’t feel like “therapy” but still support development in meaningful ways.
One such therapy is Aquatic therapy. Aquatic therapy uses water as it has a calming effect. It slows movements, softens sensory input, and creates a safe space where children can explore their bodies, emotions, and interactions at their own pace.
Hence, more and more parents are now opting for aquatic therapy for autism. In this article, we look into the details of aquatic therapy for autism, how it works for autistic kids, and its benefits.
What Is Aquatic Therapy for Autism?
Aquatic therapy for autism is also known as hydrotherapy. This type of therapy is a form of physical therapy conducted in a warm, shallow pool. It is not about learning strokes or swimming laps. It is, in fact, a structured therapeutic intervention.
Trained professionals, such as an occupational therapist, physiotherapist, or adapted aquatics specialist, guide autistic kids throughout the sessions. Aquatic therapy is often confused with autism swimming therapy; however, the two concepts differ.
It is known to use the unique properties of water, including buoyancy, resistance, and sensory input, which help children with autism to:
Improve balance, coordination, and motor planning
Regulate sensory processing and emotional responses
Build body awareness and confidence
Encourage social interaction and communication in a low-pressure setting
Aquatic therapy for autism feels less demanding and more enjoyable because the water reduces gravity’s impact, slows movement, and provides consistent sensory feedback.
In essence, aquatic therapy for autism combines the principles of sensory integration, physical rehabilitation, and play-based learning, making it a powerful complementary approach within a holistic autism intervention plan.
How Is Aquatic Therapy for Autism Performed?
Aquatic therapy for autism has a structured approach in a controlled pool environment. The activities are adapted to each child’s sensory profile, developmental level, and therapy goals.
It is a gradual process and performed in the following way:
1. Initial Assessment and Goal Setting
The first step involves evaluating the child’s sensory processing needs, motor skills, balance, emotional regulation, comfort with water, communication and social interaction skills.
Based on this assessment, individualised goals are set. It is similar to occupational therapy planning, which aims to ensure the child’s needs remain central.
2. Water Orientation
The next step involves slow and reassuring exposure to water. It can include simply sitting at the edge of the pool, splashing hands and feet, or a supported entry into the shallow side of the pool. This greatly helps children who are in for the first time.
It helps build trust, especially for children with autism who are sensory-sensitive.
3. Therapeutic Movement and Sensory Activities
As the child gets comfortable, goal-based sensory activities are introduced. It includes activities such as:
Floating or supported walking for balance
Pushing or pulling water to build strength
Reaching, kicking, or coordinated movements for motor planning
4. Play-based Interaction
Therapists use balls, toys and simple games to support guided play for an autistic child. It helps improve joint attention, turn-taking, eye contact, and the ability to follow instructions.
Children with autism can engage more when the environment feels relaxed and less demanding.
5. Cool-down and Relaxation
To ensure the child does not feel overwhelmed, the sessions are not abruptly ended. The therapist plans to end the session with relaxing activities. Activities include:
Gentle floating
Slow movement
Deep-pressure input from water
Through such relaxing activities, the child feels calm and regulated when they leave the pool.
Why Do Autistic Kids Like Water So Much?
Studies have shown that kids with autism respond positively to aquatic therapy. This makes many parents wonder: Do autistic kids like water? The answer is yes, children with ASD love water.
But here is a deeper question that parents must understand: Why do autistic kids like water? Here is the explanation for the same:
Water Offers Predictable Sensory Input
For many autistic children, the nervous system is easily overwhelmed. Water provides a very consistent, gentle pressure throughout the body. It helps in delivering calming proprioceptive input.
Deep pressure helps the brain understand the body’s position in space, leading to a sense of security and calm. It is one of the primary answers to the question: Why do autistic kids like water?
Movement Inside the Water Feels Safer
As water reduces the effects of gravity, the body feels lighter, and movements are slower and more controlled. The kids are safe, and there is less fear of falling or losing balance.
For children who struggle with coordination or motor planning, water allows them to move with greater confidence, which answers the common question: Do autistic kids like water because it feels less demanding? The maximum answers from parents is yes.
Reduced Sensory Overload
In a normal scenario, an autistic child has to manage visual input, noise, touch, and movement simultaneously on land. However, when they are in water, the:
External sensory input is softened
The environment feels more predictable
Distractions are reduced
The sensory quiet that the child feels explains why autistic kids like water. Children thus engage more willingly in aquatic activities than in busy or noisy settings.
Water Allows Freedom Without Any Pressure
When in water, there are no strict rules; the child is not expected to behave in a certain way. This freedom encourages spontaneous play, exploration, and interaction, without pressure.
Water Supports Emotional Regulation
By nature, the water has a calming effect on our nervous system. Research shows that rhythmic movement in warm water can significantly reduce stress as well as anxiety, which can help an autistic child regulate emotions. It can also help to improve focus and attention.
How Aquatic Therapy Benefits Autistic Children?
Aquatic therapy has gained significant attention in the past few years due to its immense benefits. This therapy works simultaneously with the child’s body and nervous system.
The aquatic environment creates a supportive, calming, and engaging space where children can move, learn, and interact with less pressure than they often experience on land.
Here are the benefits of autism swimming therapy for autistic children:
1. Supports Sensory Regulation
Children with autism tend to have difficulty processing sensory information, such as touch, movement, and body awareness. Water helps to organise these sensory signals. This sensory regulation is one of the strongest reasons aquatic therapy for autism is effective, especially for children who are easily overwhelmed in busy environments.
2. Improves Gross Motor Skills and Coordination
The impact of water on gravity not only makes movement easier but also allows children to practise motor skills without fear of falling. Aquatic therapy for autism helps improve balance and postural control, muscle strength and endurance, and bilateral coordination, motor planning, and body awareness.
3. Reduces Anxiety and Encourages Emotional Regulation
The calming effect that water has on the human body helps an autistic child in more ways than one. Here is how it helps:
Reduced anxiety and hyperactivity
Fewer emotional outbursts or meltdowns
Improved ability to self-soothe
Better tolerance for transitions and change
4. Better Attention, Focus and Cognitive Engagement
Aquatic therapy sessions are structured yet playful, which helps children stay engaged without feeling pressured. It helps improve the child’s overall attention span, enhances the child’s ability to follow instructions through, increases task persistence, and motivates the child to participate more.
5. Increases Self-Confidence and Independence
When the autistic child feels they can float independently, move freely, and complete tasks on their own, they feel more confident. Over time, it can help the child improve their self-esteem.
They are more willing to try new activities and give them greater independence in movement and play. This sense of achievement can positively influence participation in other therapies and daily activities.
6. Supports Behavioural Regulation
The regulation achieved in water often carries over into everyday routines. Children are known to have the following benefits:
Better sleep patterns
Improved ability to handle sensory challenges
Reduced aggression or withdrawal
Increased adaptability in new environments
This makes aquatic therapy for autism a valuable part of a holistic intervention plan.
7. Offers an Autistic Child an Enjoyable Environment
Aquatic therapy does not necessarily feel like normal therapy. It feels less clinical, which makes it more enjoyable. The risk of injury is lower, there is natural resistance without strain, and there is also a positive association with therapy.
This increases consistency and long-term participation, which is essential for meaningful progress.
Is Aquatic Therapy Safe for Autistic Children?
It is natural for parents to wonder if aquatic therapy is safe for their autistic child. However, when delivered correctly, aquatic therapy for autism is considered safe as well as well-tolerated.
It is safe when offered by a trained professional in a controlled environment with proper safety protocols in place. In fact, water-based therapy is often safer than many land-based physical activities because water naturally supports the human body and reduces the risk of injury.
Here are some other reasons why autism swimming therapy is considered safe for autistic children:
1. Professional Supervision and Clinical Oversight
Aquatic therapy is provided by certified aquatic therapists or physiotherapists trained in water-based interventions. The therapist continuously monitors the child’s physical movement, fatigue level, and emotional and sensory responses, and adjusts them to keep the child comfortable and safe at all times.
2. Water Can Reduce Impact As Well As Injury
Water provides buoyancy, significantly reducing body weight and joint pressure. It puts minimum strain on muscles and joints. For children with low muscle tone, poor coordination, or delayed motor skills, this makes autism and swimming therapy a safer option compared to many land-based exercises.
3. Controlled and Sensory-friendly Environment
Aquatic therapy sessions are conducted in carefully controlled pool settings, not public swimming areas. The pools are mostly shallow to avoid risks. Moreover, minimum noise and visual distraction are avoided.
4. Individualised Assessment Before Therapy Begins
Aquatic therapy starts with a detailed assessment of medical history, sensory sensitivities and triggers, and comfort level. This assessment helps identify any risks and ensures therapy is customised to the child’s specific needs.
In case a child has medical conditions like epilepsy, respiratory issues, or significant water-related anxiety, medical clearance is sought. Also, modified activities and one-on-one supervision are provided in such cases.
5. Low Child-to-therapist Ratios
To ensure close supervision, aquatic therapy programs usually maintain one-to-one or small-group sessions with multiple trained staff present. This allows therapists to respond quickly if a child becomes overwhelmed, tired, or distressed.
6. Emergency Preparedness
Reputable aquatic therapy programs follow strict safety standards, such as:
Emergency response training
Lifesaving and first-aid certification
Clear pool safety rules
Secure pool access and boundaries
These measures ensure quick and effective responses in the unlikely event of an emergency.
7. Parental Involvement and Communication
For safety and to ease parents’ nerves, parents are asked to observe sessions, share feedback on the child’s responses, and reinforce any safety rules or routines as needed.
These measures ensure quick and effective responses in the unlikely event of an emergency.
Conclusion
Autism Spectrum Disorder cannot be cured, but it can be managed with early intervention and timely therapy. Several therapies can be very helpful. However, considering how overwhelmed an autistic child can feel, aquatic therapy for autism is one of the best therapies to try. It is quite safe, as it is conducted by a trained therapist in a controlled environment.
By using the natural properties of water, autism and swimming therapy create an environment where children feel supported rather than overwhelmed, allowing meaningful progress through movement and play. It is a powerful tool that can help autistic children build confidence, regulation, and everyday functional skills.
Frequently Asked Questions
How is aquatic therapy different from regular swimming lessons?
Unlike swimming lessons, autism and swimming therapy focus on therapeutic goals such as balance, coordination, sensory integration, and emotional regulation rather than teaching swimming strokes or endurance.
At what age can autistic children start aquatic therapy?
Most children can begin autism and swimming therapy around 3 to 4 years of age, depending on developmental readiness, medical clearance, and comfort with water.
Can aquatic therapy help with sensory issues in autism?
Yes. Aquatic therapy for autism provides consistent tactile, vestibular, and proprioceptive input, supporting sensory integration and helping reduce sensory defensiveness and overstimulation.
Does aquatic therapy improve motor skills in autism?
Yes, water-based therapy supports improvements in balance, coordination, muscle strength, endurance, and motor planning while reducing the physical strain often experienced on land.
Do autistic kids like water?
Many autistic children enjoy water because it provides predictable sensory input, reduces sensory overload, and helps them feel calm and secure.
For expert insights, support services, and inclusive learning initiatives, visit the India Autism Center.
Sound therapy helps to improve focus, sensory processing, communication, and emotional regulation using specially designed music or frequencies. But does it really work?
In this article, we will explore what sound therapy for autism is, its different types, benefits, and how it works.
What is Sound Therapy?
What is sound therapy? Well, it is a therapeutic approach that uses specific sounds, music, or frequencies to influence brain activity, emotional state, and sensory processing.
The concept of sound therapy is based on the brain’s direct response to auditory input. As part of sound therapy, targeted sound exposure can help in:
Regulating sensory overload
Improving attention and focus
Enhancing emotional balance
Supporting speech and communication
Sound therapy is a non-invasive, drug-free, play-based approach in which structured auditory input may help gradually reshape how sound is perceived and responded to.
However, it is important to note that sound therapy for autism is a complementary therapy and is not a replacement for evidence-based interventions such as ABA, speech therapy, or occupational therapy.
Why Sound Plays a Powerful Role in Autism?
To completely understand the concept of sound therapy for autism, it is necessary to understand how sound affects the autistic brain. Through several studies over the years, many autistic individuals often experience:
Extreme sensitivity to noise
Difficulty filtering background sounds
Overreaction to sudden noises
Distress in crowded or echo-filled spaces
Auditory defensiveness
Although there have been cases where some autistic individuals actively seek intense sound stimulation, it involves repeating noises, tapping objects, or humming continuously.
The reason why autistic people have auditory sensitivity is that autism affects:
As a result, sound tends to feel painful, confusing, overwhelming, and excessively stimulating. This is exactly why autism sound therapy focuses on gradual, controlled, and therapeutic exposure to sound, helping the brain regulate its auditory responses over time.
How Does Sound Therapy Work on the Brain?
So, how does sound therapy for autism work? At the neurological level, it works through three core mechanisms:
Level 1: Neuroplasticity
Repeated exposure to structured sound helps the brain form new neural pathways. It thus helps in improving how sound is processed in the brain.
Level 2: Sensory Integration
Sound therapy also aims to strengthen communication between the auditory system and other sensory systems (touch, vision, balance).
Level 3: Emotional Regulation
Soothing sounds happen to activate the parasympathetic nervous system. It helps to reduce anxiety and emotional distress.
The three mechanisms together make the autism sound therapy work wonders. It supports:
Emotional calmness
Improved attention
Reduced sensory overload
Better behavioural regulation
What are the Different Types of Sound Therapy For Autism?
Autism can not be cured with a single treatment; it involves multiple therapeutic approaches that use sound, music, or controlled auditory input to support sensory regulation, emotional balance, communication, attention, and behaviour.
There are several clinically recognised types of sound therapy used for autistic individuals. Each works differently and serves different goals. Here are the top sound therapies for autism that are quite popular:
1. Music Therapy
Music therapy is the most scientifically validated form of sound therapy for autism. It is conducted by a certified music therapist using structured musical interaction, not just passive listening.
Before we move on to understand how it works, let us first understand why music is so powerful for the autistic brain:
The brain processes music in both the left and right hemispheres, activating areas responsible for speech, emotion, memory, and motor control.
Autistic individuals respond quite strongly to musical input compared to simple spoken language.
Music therapy also tends to improve social communication and emotional reciprocity in children with autism.
Here is how music therapy works for autism:
It activates multiple brain areas simultaneously.
It uses rhythm to organise the nervous system.
It supports emotional regulation without pressure.
2. Auditory Integration Training (AIT)
Auditory Integration Training is a structured type of autism sound therapy where children listen to filtered and modulated music through headphones over a number of sessions.
The aim is to improve:
Sound hypersensitivity
Noise-related anxiety
Auditory processing difficulties
Behavioural reactions to sound
AIT is one type of sound therapy, considered a complementary autism treatment rather than a primary treatment like speech or behavioural therapy. It works through three neurological principles:
Sound Filtering & Desensitisation: AIT uses modulated sound frequencies to gradually expose the auditory system to low sounds, mid-range speech sounds, and high-frequency notes.
Neuroplasticity (Brain Rewiring): Repeated exposure to filtered sound tends to activate the brain’s ability to form new neural pathways, reduce exaggerated emotional response to noise, and improve how the sound signals are processed.
Auditory System Regulation: AIT aims to stabilise communication among the auditory nerve, brainstem, and auditory cortex, as well as the brain’s emotional and behavioural centres.
3. Tomatis Method
The Tomatis Method is a form of sound therapy for autism that uses electronically filtered music and voice frequencies that improve how the brain processes sound.
Let us look at how the Tormatic method helps people with autism:
The child listens to modified classical music (like Mozart) and also filtered vocal sounds through specialised headphones.
This repeated stimulation supports neuroplasticity, helping the brain improve auditory processing and sensory integration.
The sound constantly shifts between high and low frequencies, which stimulates the auditory nerve and brain pathways.
The results are:
Improved level of listening attention and sound tolerance
Better speech clarity as well as language readiness
Regulation of emotions
Better sensory-motor coordination
4. Samonas Sound Therapy
Samonas, or Spectral Activated Music of Optimal Natural Structure therapy, is a form of autism sound therapy that uses modified classical music and natural sounds to improve how the brain processes sensory information.
So, how does this type of sound therapy work? Let us understand that:
The child listens to carefully filtered classical music and nature sounds through specialised headphones.
These sounds are adjusted to stimulate the auditory and vestibular systems (balance) and sensory integration pathways.
Sound therapy is usually delivered through structured listening programs over several weeks or months, often alongside occupational therapy.
5. White Noise & Nature Sound Therapy
White Noise & Nature Sound Therapy is a type of sound therapy for autism that uses consistent background sounds such as rainfall, forest sounds, or ocean waves. The natural sound helps calm the nervous system and aims to reduce sensory overload.
How does this sound therapy work? Here is how:
Steady background sounds create a predictable auditory environment.
The calm and steady background sounds create a predictable auditory environment.
The consistent sound activates the parasympathetic nervous system, which promotes relaxation and emotional regulation.
The results of white noise and nature sound therapy for autism show remarkable results, such as:
It improves the sleep quality.
Supports attention and focus
Creates a sense of safety and calm
Reduces sensory overstimulation, anxiety levels, and emotional outbursts.
It works best when combined with speech therapy, occupational therapy, and behavioural intervention.
What are the Benefits of Sound Therapy for Autism?
Sound therapy for autism is widely used as a complementary intervention to support sensory regulation, emotional balance, attention, and overall well-being. Although it is not a cure for autism, it does help improve daily functioning and quality of life.
Let us understand the benefits of autism sound therapy:
1. Reduces Sound Sensitivity & Sensory Overload
One of the biggest benefits of sound therapy for autism is improved tolerance to everyday sounds. Many autistic individuals struggle with loud or unpredictable noise. Sound therapy helps to:
Decreases ear-covering behaviour
Reduces panic in noisy environments
Improves tolerance to classroom and public sounds
Lowers sensory-triggered meltdowns
2. Improves Emotional Regulation
Different types of sound therapy help to calm the nervous system. It also supports better control over emotional reactions: It helps to:
Reduce anxiety
Decrease in emotional outbursts
Improve mood stability
Self-soothe in a better way
3. Better Sleep Quality
Sleep disturbances are very common in autism. Sound therapy for autism, especially white noise and nature sounds, can greatly improve sleep quality. It helps in achieving:
Faster sleep onset
Fewer night wakings
Deeper, more restful sleep
Reduced bedtime anxiety
4. Better Attention Span, Focus, and Learning Readiness
Many forms of autism sound therapy improve the brain’s ability to filter background noise. Sound therapy leads to:
Better focus during tasks
Improved classroom participation
Increased learning engagement
Reduced distractibility
5. Improves Social Engagement & Interaction
Music-based sound therapy for autism is known to encourage shared attention, turn-taking, as well as emotional connection. It offers social benefits, including:
While it cannot entirely replace speech therapy, sound therapy for autism does support the foundations needed for communication. It helps by:
Improving speech rhythm and flow
Encouraging vocal imitation
Supporting expressive communication
Preparing the brain for speech therapy progress
7. Reduces Anxiety & Stress Levels
Many individuals suffering from autism live in a constant state of sensory stress. Autism sound therapy activates the body’s relaxation response. The results are known to include:
Lower levels of stress hormone
Reduced fear responses
Greater emotional calm
Improves the adaptability to change
8. Helps with Behavioural Regulation
When sensory stress decreases, behaviour often improves naturally. Sound therapy for autism offers behavioural benefits like:
Fewer aggressive outbursts
Reduced irritability
Improved impulse control
Better frustration tolerance
9. Supports Sensory Integration & Body Awareness
Several types of sound therapy support how the body processes sensory input and improve the following:
Balance and coordination
Body awareness
Motor planning
Sensory-motor integration
10. Improves Overall Quality of Life
Considering all the benefits, it is needless to say that sound therapy for autism does lead to an improved quality of life. With sound therapy, individuals with autism can:
Feel calmer and safer.
Sleep better
Engage more socially
Learn more comfortably
Experience less emotional distress.
Does Sound Therapy Work for Autism?
There is no direct answer to the question. Yet, it is one of the most searched questions. Although sound therapy has several benefits, it still has limitations in autism treatment.
Things that sound therapy do not include:
Cure autism
Eliminate core neurological differences.
Replace behavioural or speech therapy.
Guarantee speech development
Autism sound therapy works best as a supportive, complementary intervention, but never as a standalone treatment.
When is Sound Therapy Not Suitable?
Not every autistic individual responds positively to sound therapy. Sound therapy may not seem to work if the child has:
Extreme auditory defensiveness
Sound-triggered seizures
Anxiety disorders
Trauma-related sound sensitivity
Finally, sound therapy works best when combined with other targeted therapies. Also, results may vary from individual to individual.
Conclusion
Sound therapy for autism is considered a non-invasive, gentle approach to support sensory regulation, emotional calm, and everyday functioning. While it is not a cure, it does improve the quality of life. The journey of autism care is long, and sound therapy is more than just a stimulus. Sound therapy can prove to be a powerful tool for providing comfort, connection, and steady progress for an individual with autism.
Frequently Asked Questions
What is autism sound therapy used for?
Autism sound therapy is mainly used to reduce sensory overload, improve sleep, calm anxiety, enhance attention, and support emotional regulation. It is often used alongside speech therapy, occupational therapy, and behavioural interventions.
Is music therapy the same as sound therapy for autism?
Music therapy is a clinically proven form of sound therapy for autism, but not all sound therapies are music therapy. Music therapy is therapist-led and focuses on communication and social interaction, while other sound therapies mainly target sensory regulation.
Is sound therapy for autism safe for children?
Yes, sound therapy for autism is considered to be safe, non-invasive, and drug-free when used at appropriate volumes and under professional guidance. Safety depends on the child’s sensory tolerance and proper supervision.
At what age can sound therapy for autism be started?
Sound therapy for autism can be started as early as toddlerhood, especially in early intervention programs. However, therapy choice should always be guided by a developmental specialist.
How long does sound therapy for autism take to show results?
Results from sound therapy for autism vary. Some individuals show changes in a few weeks, while others may need several months of consistent use for noticeable improvements.
For expert insights, support services, and inclusive learning initiatives, visit the India Autism Center.
As per research, several children and adults with autism spectrum disorder tend to have atypical gaze patterns. These visual differences can affect communication, learning, behaviour, and even social connections.
That is why visual therapy for autism, also commonly called vision therapy for autism, is becoming an essential support system for children and adults on the spectrum.
Today, we will uncover what vision therapy for autism is, how it works, and how it can help. We will also discuss which techniques are most effective and how visual therapy contributes to skills, such as how to improve eye contact for autism and help address autism lazy eye (amblyopia).
What Is Visual Therapy?
Visual therapy is a personalised program that helps strengthen the communication between the eyes and the brain. It’s not just about improving eyesight; it’s about improving how the brain uses visual information in daily life.
The eyes capture information, and then the brain interprets it. Vision therapy ensures it happens efficiently.
For autistic individuals, this can be life-changing because the visual system influences:
Vision therapy can be helpful as the visual skills improve, making daily tasks more manageable, smoother, and less overwhelming.
Why Visual Challenges Are Common in Autism?
Many autistic individuals experience visual-processing differences for several neurological and sensory reasons:
Neurological pathways develop differently: The brain regions responsible for visual attention, eye coordination, and face processing may grow at different paces.
Hyperfocus or difficulty shifting attention: Some children can zoom in on details but struggle to shift their gaze between objects or people.
Sensory processing differences: Bright lights, busy environments, or fast-moving visuals can make children with ASD feel overwhelmed.
Co-occurring conditions: Certain types of developmental delays, ADHD, dyspraxia, and dyslexia are known to accompany ASD, affecting visual-motor skills.
Higher rates of eye conditions: Conditions like strabismus, convergence challenges, and autism lazy eye (amblyopia in autistic individuals) are more frequent.
Everyday tasks can feel much more demanding when these factors are combined.
How Visual Therapy Supports Autistic Individuals?
Visual therapy is more than just an eye check-up and some random exercises. Vision therapy for autism focuses on:
Strengthening eye muscles
Better focus
Encouraging smooth gaze shifting
Teaching the brain to process visual signals correctly
Reducing visual overload
Ensuring that coordination between body movement and vision is enhanced
Enhancing comfort in busy visual environments
Who Can Benefit from Visual Therapy for Autism?
When the proper technique and visual therapy for autism are used, it can help children with autism spectrum disorder to live a better life. It is especially valuable for:
Children avoiding eye contact
Kids who lose their place while reading
Children who seem “clumsy” or bump into objects
Kids with handwriting difficulties
Children who tilt their heads to look at objects
Those diagnosed with autism lazy eye
Children with sensory overload or anxiety driven by visual input
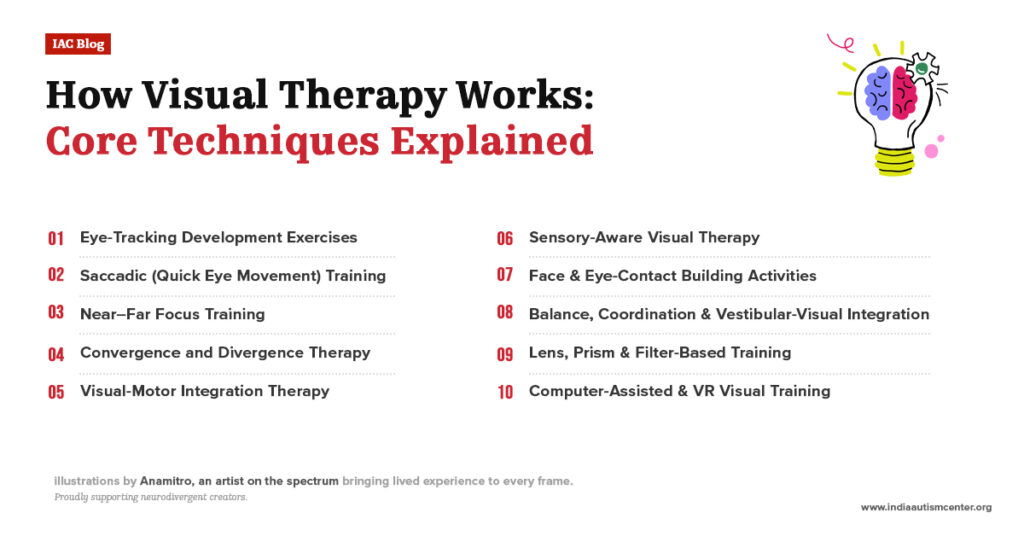
How Visual Therapy Works: Core Techniques Explained
Visual or vision therapy for autism uses structured, engaging, and purposeful activities to improve the visual system. These exercises are often fun and play-based, which helps keep children motivated. If you are wondering how to improve eye contact for autism, then here are the most effective therapies that are widely used:
1. Eye-Tracking Development Exercises
These exercises teach the eyes to follow objects smoothly, as many autistic children struggle with tracking, leading their eyes to jump rather than move smoothly. It can cause problems such as difficulty copying from a board, losing place while reading, challenges with playing sports, or poor eye contact.
For this exercise, the therapists use tools like:
Moving light pens
Tracking balls
Bubbles
Flashlight following
Computer-based eye-tracking games
These exercises teach the eyes to track objects accurately, making reading and conversation much easier.
2. Saccadic (Quick Eye Movement) Training
The term “Saccades” refers to the quick jumps your eyes make between two points. Children with saccadic difficulties may come across as inattentive, or they may be prone to losing information. Therapists use:
Word-jump charts
Dot-to-dot eye jumps
Rapid pointing games
This helps improve classroom performance and conversation flow.
3. Near–Far Focus Training
Shifting the focus from near objects to far objects can often be difficult for people with ASD. Thus, training can be helpful for school tasks such as switching between a book and a board.
The tools used for this exercise include:
Near-far charts
Focus cards
Digital focus training apps
This training is particularly helpful for children who experience headaches or fatigue due to frequent visual shifts.
4. Convergence and Divergence Therapy
When the eyes don’t work as a team, children may see double or feel visually confused. This vision therapy for autism helps to ensure that both eyes work in coordination. This is also the main therapy used for lazy eye in autism.
Therapists use:
Brock String
Barrel cards
3D stereoscope training
Dot fusion cards
It helps strengthen binocular vision, improve depth perception, enhance sports performance, and reduce blurry vision.
5. Visual-Motor Integration Therapy
Visual-motor integration is important for several day-to-day activities, such as writing, eating independently, buttoning, hand-eye coordination, and participating in sports. As part of this visual therapy for autism, therapists use tools like:
Pegboards
Maze tracing
Craft activities
Ball-catching
Pattern copying
Tracing worksheets
This helps children coordinate what they see with what their hands do.
6. Sensory-Aware Visual Therapy
Many autistic children find bright lights, crowds, or fast visuals overwhelming. This vision therapy technique for autism aims to help children who struggle with visual overload.
As per this technique, the therapist creates a sensory safe environment using:
Low lighting
Contrast-based activities
Visual-motor calming tasks
Slow-eye movement exercises
Visual schedules
It helps reduce stress, improve the overall attention span, and keep children regulated.
7. Face & Eye-Contact Building Activities
Several autistic children tend to avoid eye contact, not out of defiance, but because it feels uncomfortable or overwhelming. As a parent seeking to know how to improve eye contact in autism, this technique can be quite helpful.
The therapy will include the following:
Joint Attention Games: Pointing, showing, and sharing toys.
Mirror Play: Helps children look at faces without pressure.
Gaze-Following Activities: Teaching children to follow someone’s eyes to understand attention.
Naturalistic Play: Positioning toys near the therapist’s face so the child naturally glances at them.
Children with visual-processing differences may also have difficulties with balance or body awareness. The therapy aims to ensure that vision and movement work together. The treatment includes different tools, such as:
Balance boards
Trampolines
Obstacle courses
Body tracking games
When the visual and vestibular systems align, children become more confident and coordinated.
9. Lens, Prism & Filter-Based Training
This technique is also used to treat autism lazy eye, and reading difficulties. It is used only by developmental optometrists. The special lens and prism help to:
Align the eyes
Improve focus
Reduce visual stress
Enhance attention
Support depth perception
10. Computer-Assisted & VR Visual Training
These exercises are engaging, motivating, and highly effective for older children and teens. Technology-based training is now widely used:
Interactive VR visual tasks
Eye tracking software
Attention shift games
Binocular VR games
Benefits of Visual Therapy for Autism
Visual therapy for autism offers several benefits, as the visual system influences communication, learning, motor skills, and emotional regulation. Here are the benefits of vision therapy for autism.
Improved Eye Contact & Social Engagement
One of the most common questions parents ask is how to improve eye contact for autism. Visual therapy supports this by strengthening eye tracking, gaze shifting, face processing, joint attention, and visual comfort during conversation.
Children gradually begin to:
Look toward a person’s face more naturally
Maintain brief eye contact without distress
Understand where others are looking
Respond better to name-calling and facial cues
Stronger Reading, Writing & Academic Skills
After visual therapy for autism, improvements often include:
Better tracking across text
Improved reading fluency
Accurate copying from the board to the notebook
Stronger letter formation
Better spacing and writing alignment
Reduced Sensory Overload & Visual Stress
Some autistic individuals experience visual hypersensitivity to bright lights, screen glare, and crowded environments, which may feel overwhelming. Visual therapy will help to:
Filter unnecessary visual information
Reduce overstimulation from movement
Improve visual attention span
Stay calmer in busy spaces
Better Motor Skills & Body Awareness
Vision guides body movement, so when the visual system becomes stronger, physical coordination also improves. The benefits of vision therapy for autism include:
Better balance
Smoother walking/running
Improved ball skills
Stronger hand-eye coordination
More confidence on playgrounds
More Independence in Daily Tasks
Parents often report noticeable improvements in daily functioning within months in terms of:
Eating
Buttoning and zipping
Sorting objects
Using tools correctly
Completing homework independently
What Is Autism Lazy Eye & How Does Visual Therapy Help?
Autism lazy eye, or amblyopia occurs in autistic individuals. Amblyopia means one eye is weaker and sends fewer signals to the brain. Children with autism are more prone to have this condition due to:
Inconsistent gaze
Difficulty maintaining eye alignment
Tracking issues
Sensory avoidance of visual tasks
How does Visual Therapy treat Autism Lazy Eye?
Visual therapy helps the brain reconnect with the weaker eye, restoring binocular vision and preventing long-term sight loss. Therapy techniques include:
Strengthening the weaker eye
Teaching both eyes to work together
Prism therapy to improve alignment
Focus-shifting activities
Binocular games
3D stereoscopic exercises
Patching (when prescribed)
Signs Your Child Might Need Visual Therapy
It is easy to assume that your child’s vision is perfect if they can see clearly. But visual-processing challenges are often hidden and may go undetected during a routine eye exam.
Children who have ASD often struggle with tracking, focusing, depth perception, or eye coordination without being able to explain what feels difficult. Here are some signs that you must look out for to understand if your child needs vision therapy:
Mirror Imitation Games: Great for early social referencing and face awareness.
Sensory-Friendly Visual Spaces: Soft lighting, clear labels, and contrast-rich visuals aim to help reduce overload.
Conclusion
Vision impacts every aspect of humans, and it is the same for children with ASD, whether it is reading and writing, eye contact, social connection, or staying regulated in sensory-rich environments. Visual therapy has been shown to deliver powerful, life-changing results.
By strengthening the communication between the eyes and the brain, vision therapy aims to help autistic individuals see, process, and respond to the world in a more comfortable way. Families who opt for structured and evidence-based visual therapies and treatment, especially through integrated centres, see remarkable progress in confidence, communication, learning, and daily independence.
Frequently Asked Questions
What is visual therapy for autism, and how does it work?
Visual therapy, also known as vision therapy for autism, is a structured program that improves coordination between the eyes and the brain. It uses exercises that strengthen tracking, focusing, eye coordination, and visual processing. Over time, children learn to interpret visual information more efficiently, which positively impacts reading, writing, social skills, and daily activities.
Can visual therapy help my child improve eye contact?
Yes. Many children avoid eye contact due to visual discomfort, not behavioural resistance. Through gentle gaze-shifting exercises, face-tracking tasks, and sensory-supported techniques, visual therapy supports the natural, pressure-free improvement of eye contact for autism.
Does vision therapy help with lazy eye in autism?
Yes. Autism lazy eye (amblyopia in autistic children) is treatable through visual therapy. Therapists strengthen the weaker eye, improve binocular vision, and retrain the brain to use both eyes together. It helps to improve depth perception and reduce long-term visual imbalance.
How long does it take to see results from visual therapy?
Most parents notice improvements within 8–12 weeks. However, children with significant visual-processing challenges or autism lazy eye may need 6–12 months of consistent therapy. Progress depends on regular sessions and home reinforcement.
Looking for expert support and inclusive learning options? Contact India Autism Center.
These facts make one thing for sure: The families of disabled persons are not always lacking support; they are, in reality, lacking access to information.
Whether you’re a caregiver of a child with autism, someone with a locomotor disability, or an adult seeking financial independence, this guide ensures that you not only know the schemes but also fully understand how they can improve your daily life.
Today, we will provide a detailed, up-to-date list of government schemes for persons with disabilities in India.
The Complete List of Government Schemes for Disabled Persons in India (2026)
Finding the right support for disability can be quite overwhelming. Several disabled persons and their families are missing out on available government support. This updated list of government schemes for persons with disabilities in India (2026) brings together all major welfare initiatives.
Especially when you are the parent or a primary caregiver of a kid who has autism spectrum disorder, an adult with a disability, or a caregiver who is looking for proper guidance, this guide simplifies the landscape so you can finally understand and claim the support you deserve.
1. NIRAMAYA Health Insurance Scheme – Healthcare Safety Net
When it comes to support for people with disabilities, health insurance is more than just an option; it is a necessity, a health insurance scheme exclusively for PwDs that provides coverage for a wide variety of medical needs.
There is no need for pre-insurance medical tests. Irrespective of age or disability type, there is only one time premium. This ensures that medical emergencies don’t become financial disasters.
Transportation costs associated with care or treatment
Who Can Apply:
Persons with disabilities (autism, cerebral palsy, intellectual disability, multiple disabilities) with a valid disability certificate and UDID/enrollment number.
2. VIKAAS Daycare Scheme – Daytime Care, Therapy & Skill Building
Besides early intervention, children with disabilities can benefit from schemes like day care. There are daycare centres run by certified organisations that aim to provide therapy, education, and social & life-skills training during daytime hours.
For families seeking assistance for disabled persons while balancing other responsibilities, VIKAAS ensures children get needed support without needing full-time institutionalisation.
What the Scheme Covers:
Special educators and therapy support
Physiotherapy / occupational therapy for mobility or daily-living support
Counselling & skill-building to improve communication, daily living, and social skills
Structured environment for growth and learning during the day hours
Gives family members respite while ensuring the child’s growth and learning
Who Can Apply:
Children/young persons (10+ years), with autism, cerebral palsy, intellectual disability, or multiple disabilities. The applicant mustn’t already be enrolled in other residential schemes such as GHARAUNDA or SAMARTH.
3. GHARAUNDA (Group-Home for Adults) – Long-Term Care & Support
GHARAUNDA is a scheme that provides a safe, lifelong group home for adults with disabilities under the umbrella of the relevant national disability legislation.
It is one of the most stable government facilities for disabled persons, ensuring long-term inclusion, dignity, and independence for adults who may not be able to live independently.
What the Scheme Covers:
Secure residential home providing 24/7 care.
Access to medical care, therapy, physiotherapy/occupational therapy.
Special educators, vocational/pre-vocational training for skill development.
A structured, supportive environment that helps people build daily living and vocational skills, social interaction, and meaningful routine.
Who Can Apply:
Adults (18+ years) with disabilities such as autism, cerebral palsy, intellectual disability, including intellectual retardation, or multiple disabilities.
4. SAMARTH Respite & Residential Care – Temporary Shelter and Support
SAMARTH aims to offer residential or respite care and assistance for disabled persons; it is particularly helpful for orphans, abandoned persons, PwDs from low-income backgrounds, or families in crisis. It serves as a critical government facility for people with disabilities, offering meaningful respite, especially when family support is absent or temporary relief is needed.
What the Scheme Covers:
Group-home style living with basic medical care
Support from special educators, vocational trainers, therapists (physio / occupational) to improve physical functionality and daily-living skills
Periodic assessments can help to monitor progress and offer tailored support plans
Safe, caring environment for those needing temporary or long-term residential support
Who Can Apply:
Persons with autism, cerebral palsy, or other disabilities, as per the relevant disability act, especially those not under other long-term or daycare schemes for disabled people in India, such as Disha, Vikaas, or Gharaunda scheme, are at the same time.
This is a flagship centrally sponsored program that aims to support NGOs/voluntary organisations that work for PwDs. DDRS helps build infrastructure and services for rehabilitation and inclusion through financial grants and other forms of aid.
By funding grassroots organisations, DDRS strengthens the network of government facilities for people with disabilities across the country, thereby increasing reach, quality, and sustainability.
What the Scheme Covers:
Establishment and maintenance of special schools, vocational training centres
Early intervention centres for children with developmental delays
Infrastructure improvements (ramps, toilets, and other accessible facilities) are made in disability-support institutions.
Community-based rehabilitation and inclusive social initiatives
Who Can Apply:
NGOs must be registered under the PwD Act/Trusts Act/Societies Act and must have at least 2 years of experience delivering disability-related services. They must also meet the government’s infrastructure, staff, and service-quality standards to receive funding.
6. SAHYOGI Care-Associate Training Scheme – Skilled Caregiver Training
A training scheme that builds a network of trained caregivers (care associates) across India to support PwDs and their families. By enhancing the availability and quality of care, this scheme for disabled people in India significantly enhances day-to-day support, enabling PwDs to lead more independent, dignified lives, and reduces the burden on families.
What the Scheme Covers:
Basic (3-month) and advanced (6-month) courses covering first-aid, basic care, communication skills, special needs support (for autism, CP, etc.)
Paid internships/placements, enabling livelihood opportunities while meeting demand for caregiving professionals
Empowers families by offering professional-grade care support, especially beneficial when managing severe disabilities
Who Can Apply:
People aged roughly 18 to 35 years, with a minimum of 8th-grade education, who wish to become care associates. Also aimed at parents/guardians seeking training.
7. Indira Gandhi National Disability Pension Scheme (NSAP) – Financial Support for Vulnerable Adults
A pension scheme offering monthly financial aid to adults (18–79 years) with severe disabilities (≥ 80%) and living below the poverty line (BPL), helping them meet basic needs.
This is a foundational social security net, a core example of how the Indian state provides assistance for disabled persons who are economically marginalised, allowing them dignity and basic financial support.
What the Scheme Covers:
Monthly pension (for example, ₹300 for eligible adults). The amount may be higher for those aged 80 or older.
Basic financial security for those unable to work due to disability
Who Can Apply:
The applicant must be a person with a severe or multiple disability (typically 80% or above), and belong to a household under the Below Poverty Line (BPL) classification.
The eligible age group is 18 to 79 years (some state-specific norms may apply).
8. Welfare Schemes for Persons with Disabilities – Allowances, Incentives, Scholarships & Travel Support
This is a government scheme in India for people with disabilities that offers multiple welfare benefits to improve financial security, social inclusion, and access to opportunities for PwDs.
These schemes give real-world, everyday assistance for disabled persons, helping them lead a dignified life with social participation, mobility, education, and financial stability.
What the Scheme Covers:
A one-time amount (for example, ₹30,000) to support disabled persons upon marriage, acknowledging their right to a dignified social life.
A monthly maintenance grant is provided (e.g., ₹1,500) for individuals with certain disabilities that can help them with everyday needs.
An annual scholarship (₹3,000–₹8,000 or more) for disabled students ensures continuity in education.
Free or subsidised public transport for PwDs holding a valid disability certificate improves mobility and access.
For unemployed persons with disability (meeting certain criteria), a small stipend (e.g., ₹400–₹1,000/month) is offered to support basic needs while they seek work or training.
Who Can Apply:
Applicants need to have a disability certificate. For unemployment allowance, the applicant must be aged 18 to 48, registered as unemployed, and have a 10th-grade education.
9. ADIP Scheme (Full Form – Assistance to Disabled Persons for Purchase/Fitting of Aids & Appliances) – Assistive Devices & Mobility Support
ADIP helps persons with disability acquire essential certified aids and appliances which can help in enhancing mobility, independence, communication, and daily living capabilities. For many PwDs, assistive devices are a gateway to independence.
ADIP brings those within reach, thereby reducing caregivers’ burden and increasing the person’s ability to lead a more self-reliant, active life.
Hearing aids, assistive devices for speech/communication (very relevant for autism/intellectual disability)
Visual aids, prosthetics, mobility supports
Pre-aid surgeries or procedures when required for proper use of devices (e.g., orthopaedic)
Who Can Apply:
Indian citizens with at least 40% disability, certain income thresholds, and who have not received similar assistance in recent years.
10. BADHTE KADAM – Awareness, Inclusion & Community Sensitisation Programme
BADHTE KADAM is a scheme to promote social awareness, community interaction, and inclusion of PwDs. It is helping change attitudes, reduce stigma, and build inclusive societies.
Access to government facilities for disabled persons is only part of the journey. For real social empowerment, public attitudes must shift. BADHTE KADAM works prominently for that, making inclusion part of the mainstream social fabric, and not just some policy documents.
What the Scheme Covers:
Supports community sensitisation efforts through campaigns, workshops, and awareness drives
Encourages inclusive policies in local communities, schools, and workplaces
Spreads knowledge about disability rights, support schemes, and social inclusion
Who Can Apply:
Registered organisations (under the National Trust) working for persons with autism, cerebral palsy, intellectual disability, or multiple disabilities.
Conclusion
Disabled people need as much assistance as possible. Empowering persons with disabilities isn’t just a government responsibility; it’s a collective step that is taken toward a more inclusive India where everyone gets a fair opportunity. The government has a wide range of schemes in place offering financial aid, healthcare support, education benefits, and rehabilitation services. Every eligible individual can access opportunities to improve their quality of life.
Being aware of and understanding the key details of these schemes for the disabled in India is the first step towards accessing their benefits. Encourage, apply, and help someone claim the support they deserve. India’s progress depends on inclusion, and inclusion begins with awareness.
Frequently Asked Questions
What are the major government schemes for disabled persons in India?
There are several key disability welfare and government schemes that a person with disability can avail themselves of in India, including the Deendayal Disabled Rehabilitation Scheme (DDRS), the Indira Gandhi National Disability Pension Scheme (IGNDPS), the ADIP Scheme, Scholarships for Students with Disabilities, the UDID initiative, and Skill Development for PwDs. These schemes provide financial assistance, rehabilitation support, mobility aids, education grants, and livelihood opportunities.
Who is eligible for government disability benefits in India?
To be eligible, an individual must have a benchmark disability of 40% or more, possess a valid Disability Certificate/UDID card, and meet specific income, age, or category-based criteria depending on the scheme.
What documents are required to apply for schemes for disabled persons in India?
Common documents to apply for different government schemes for disabled persons include:
Disability Certificate or UDID
Aadhaar Card
Income Certificate
Age Proof
BPL Card (if applicable)
Bank account details
Passport-sized photographs
What is the UDID card, and why is it mandatory?
The UDID (Unique Disability ID) card creates a national registry of PwDs. It removes the need for multiple disability documents. It also ensures quick access to any scheme for the handicapped in India. With UDID, beneficiaries can apply for pensions, aids, transportation concessions, and education benefits seamlessly.
For expert insights, support services, and inclusive learning initiatives, visit the India Autism Center.
The world is always buzzing with sights, sounds, smells, and textures. Many people find it natural to process the constant stream of sensory input. However, for autistic individuals, this same sensory world can feel intense, unpredictable, or even overwhelming.
A bright supermarket light, the scratchy texture of a shirt, or the mixed smells in a food court may be enough to trigger discomfort or anxiety. It might come as a surprise to many, but food can also become a sensory experience, sometimes soothing, sometimes stressful.
It is therefore necessary to understand the autism food list. You can consider it as a personalised, balanced, sensory-aware guide that turns mealtimes from a struggle into a predictable, comforting routine.
So, let’s understand the whole concept step by step.
What Is an Autism Food List?
An autism food list is not a fixed, one-size-fits-all autism food diet. Instead, it’s a custom meal guide that focuses on:
Your child’s nutritional needs
Their sensory preferences
Their tolerance for smells, textures, and flavours
Their digestive health and energy regulation
The goal is to ensure that autistic individuals eat foods that nourish the body, calm the senses, and avoid those that may cause discomfort or overstimulation. Hence, it is essential to select a comprehensive autism care facility that focuses on providing autism diet plans curated with care.
Food Groups Helpful for Autistic Individuals
Here are the key food groups and effective autism diet lists:
Gut-Friendly Foods
Digestive health plays a major role in mood, behaviour, and overall comfort. A balanced gut often means fewer meltdowns, better sleep, and improved focus.
Why is it necessary to have gut-friendly food?
Considering that many autistic individuals experience bloating, constipation, gas, food intolerance and even disrupted gut bacteria balance, probiotic and fibre-rich food can help restore digestive comfort.
Include these in the diet:
1. Fermented Foods (great for digestion & microbiome)
Homemade curd (yoghurt)
Buttermilk
Idli & dosa batter
Naturally fermented pickles (achar)
2. Fibre-Rich Vegetables (keeps digestion smooth)
Ladyfinger (okra)
Bottle gourd (lauki)
Pumpkin
Spinach
3. Prebiotic-Rich Foods (feed good gut bacteria)
Garlic
Onions
Bananas
Foods Rich in Vitamins & Minerals
Nutrients like Vitamin B6, Vitamin C, and Magnesium can influence brain function and mood regulation; hence, they are commonly explored for autism support.
This food option can be incorporated into the autism sensory diet by:
Blending into smoothies
Making crispy chips
Stirring into dosas or parathas
Baking into muffins
Small texture changes can lead to big improvements in acceptance.
Sensory-Friendly Foods
When it comes to sensory diet for autism, the real challenge is not the flavour but the texture. Soft foods are more often considered to be safe because:
They require minimal chewing
They don’t produce loud crunch sounds
They are predictable and consistent
Options for sensory diet for autism:
Soft Carbs:
Mashed sweet potato
Boiled rice
Dal khichdi
Soft idlis
Smooth Fruits:
Bananas
Chiku
Stewed apples
Mild Proteins:
Moong dal
Paneer bhurji
Poached eggs
Nutrient-Dense Foods
For better brain development, mood stability, and energy levels, include foods that pack essential vitamins, minerals, and healthy fats.
Iron-Rich Foods:
Ragi
Rajma
Black chickpeas
Methi (fenugreek leaves)
Healthy Fats:
Coconut
Sesame seeds
Ghee
Walnuts
Vitamin-Packed Veggies:
Moringa (drumstick)
Beetroot
Carrots
Energy-Stabilizing Foods
An autism diet plan must have energy-stabilising food options, as blood sugar swings can trigger irritability, distraction, fatigue, or sudden behavioural shifts.
Helpful energy-balancing foods:
Complex Carbs:
Jowar roti
Bajra roti
Poha
Upma
Protein-Carb Mixes:
Curd rice
Dal chawal
Besan chilla
Nuts and Seeds:
Almonds
Flaxseeds
Peanuts
Sunflower seeds
How to Create an Autism Food List (Step-by-Step)
Creating the right autism diet plan is not just a routine task but a structured approach that helps manage several aspects, including nutrition, behaviour, sensory needs, and daily wellbeing.
Many parents struggle with autism food aversion, autism food sensitivity, selective eating, restricted textures, and unpredictable preferences.
Here is a step-by-step guide to help you create a practical, sensory-informed, and health-focused autism diet list while keeping individual comfort and nutritional balance in mind.
Step 1: Start With a 7-Day Observation Journal
When you start to create an autism diet list, you first have to invest some time in observing your child’s eating habits. It will help you to create a baseline for understanding diet and autism patterns.
Here are some things that you need to track:
Consistently accepted foods (autism-safe foods)
Foods causing refusal or distress (autism food refusal, autism and food aversion)
Sensory responses such as gagging, rejecting textures, or preferring only white/beige foods
Temperature and texture preferences (autism and food textures, food textures and autism)
Tracking these patterns will help to understand the core of autism food issues, identifying where food aversions, autism or autism and food selectivity are strongest. This also confirms whether food aversion is a sign of autism in your child.
Step 2: Organise Foods Into Sensory Categories
Mealtime anxiety in autistic children can be managed with a strong sensory diet for autism or an autism sensory diet. It is necessary to classify food options by sensory features rather than standard nutritional groups.
Sensory-based categories:
Crunchy foods
Soft/pureed foods
Liquids & smooth foods
Warm vs. cold foods
Low-odor foods
Categorising by sensations helps align your sensory diet for autism with daily meals. It also helps address food aversions and autism, particularly when a child rejects foods based on smell, texture, or appearance.
Step 3: Identify “Safe Foods” and “Maybe Foods”
The foundation of the autism-friendly foods section in your final chart is incomplete without understanding which foods are safe.
These are eaten without resistance and can be used to anchor meals.
Maybe Foods
These are foods accepted occasionally or under specific conditions.
It is important to understand the difference to reduce stress during meals. It will be quite helpful in creating a structure for your personalised autism food plate or autism-safe food framework.
Step 4: Add Sensory-Compatible Alternatives
After identifying safe food, it is now time to introduce similar sensory alternatives. This prevents nutritional gaps while respecting autism and food sensitivities.
Examples:
If crunchy foods are preferred: roasted chickpeas, veggie sticks
If smooth foods are preferred: pureed soups, blended porridges
If warm, bland foods are preferred: soft rice, khichdi
This step supports gradual progress in tackling autism-related food aversion, food refusal, and food selectivity.
Step 5: Build a “Restricted Foods” List
Along with other important considerations like safe foods for autism, maybe foods, and sensory-compatible foods for autism. It is equally important to recognise the foods to avoid for people with autism.
The food options that you must keep in the restricted autism food list include:
Allergic reactions (autism and food allergies)
Digestive discomfort
Sensory overload
Behavioural triggers
Here are some examples for you:
Artificial dyes
Highly processed snacks
Foods with strong smells
Certain dairy or gluten items, depending on sensitivity (autism and gluten-free diet)
Knowing which foods to avoid with autism helps ensure the autism diet plan remains supportive and consistent.
Step 6: Balance the List With Nutrition Categories
A proper diet for autism spectrum disorder must consider nutrition, sensory needs, and health conditions.
Nutrients that are essential in an autism diet plan include:
Proteins
Carbohydrates
Fruits
Vegetables
Fats
As a parent, you can explore diet options such as:
Gluten-free diet for autism
GAPS diet autism (Gut and Psychology Syndrome diet)
Keto diet and autism, or autism and ketogenic diet
Step 7: Create Visual Meal Planners Based on the Autism Diet List
Meal planners help to support predictability and reduce anxiety.
Some examples of visual tools include:
Picture-based autism food plate
Weekly charts using food images
Step-by-step meal sequences
Colour-coded portion guides
These tools reinforce structure and help the child engage better with their autism-friendly foods.
Step 8: Review and Update Every 30 Days
Even the best plans take time, as eating preferences often evolve. Here are the steps you can take:
Recheck:
Newly accepted foods
New sensory challenges
Increasing or decreasing levels of autism food sensitivity
Updated notes on autism and food textures
This ensures your autism diet list and autism nutrition diet stay relevant and supportive.
Important Components for Your Autism Diet Chart
A meal that feels routine to others can become overwhelming when strong smells, unexpected textures, or loud surroundings mix with heightened sensory sensitivity.
“The moment I stepped in, the heavy aroma of food filled the air, overwhelming my senses. The greasy dishes on display felt like they were closing in on me, while the clatter of trays and the hum of conversations grew deafening. Panic took over, my chest tightened, my legs refused to move, and tears spilt down my face. My mother’s voice reached me, full of concern, but I couldn’t respond. She carried me home. Tomorrow was another day.”
Stories like this are evidence of why an autism diet chart can have a considerable impact.
The right food choices not only add nutrition but also bring comfort, predictability, and calm.
Balanced meals can:
Reduce sensory discomfort
Support digestion and reduce anxiety
Improve focus and energy stability
Minimise meltdowns triggered by food textures or smells
A well-designed chart also helps you identify what foods to avoid with autism, like:
Highly processed snacks
Strong-smelling or intensely flavoured foods
Hard-to-chew textures
Fruits and Vegetables for Brain and Gut Health
Food directly influences attention, mood, and digestion, three areas many autistic individuals struggle with. Adding nutrient-dense produce to the autism diet chart strengthens both brain and gut function.
What it Essentially Helps With
Berries protect brain cells and improve memory.
Oranges boost immunity and support cognitive health.
Spinach and kale provide iron and folate to support better concentration.
Broccoli and cauliflower can aid in detoxification and support gut strength.
Carrots and bell peppers increase immunity with beta-carotene.
Quick Reference Table
Food
Benefit
Blueberries
Protects brain cells, boosts memory
Spinach
Provides iron for energy and focus
Oranges
Enhances immune + brain function
Broccoli
Supports gut health + detoxification
Fibre-Rich Choices for Better Digestion
Digestive issues, including constipation, gas, or bloating, are quite common in individuals with autism. A fibre-rich section in your autism diet chart helps manage this discomfort and promote regular bowel movements.
Why Fibre Matters
Supports smoother digestion
Feeds healthy gut bacteria
Reduces inflammation
Prevents constipation
Top Fibre-Boosting Foods
Apples can help in nurturing good gut bacteria
Bananas improve digestion with soluble fibre
Sweet potatoes deliver prebiotic fibre
Brussels sprouts reduce inflammation and aid detoxification
Quick Reference Table
Food
Provides soluble fibre, aids digestion
Apples
Feeds gut bacteria, prevents constipation
Bananas
Provides soluble fiber, aids digestion
Sweet Potatoes
Supports gut health with prebiotics
Brussels Sprouts
Reduces inflammation + detoxifies
Nutrient-Dense Foods for Stable Energy & Mood
Energy crashes and sudden mood swings often have a nutritional root. Including slow-release, nutrient-dense foods in an autism diet chart supports stable energy levels and reduces irritability.
How These Foods Help:
Apples and berries provide slow-release natural sugars
Bananas stabilise nerve and muscle function
Carrots and squash offer long-lasting carbohydrates
Spinach and bell peppers supply magnesium to calm the nervous system
Quick Reference Table
Food
How It Helps
Apples
Provides steady energy release
Bananas
Regulates nerve + muscle function
Carrots
Slow-digesting carbs for sustained energy
Spinach
Magnesium-rich food that reduces hyperactivity
Thinking About Starting an Autism-Friendly Diet? Start Here.
When you are thinking of creating an autism-friendly diet. It doesn’t need to have complicated restrictions. It is more important to understand your child’s sensory world and their relationship with meals.
Here is how you can begin:
Observe sensory triggers: Which smells, textures, or temperatures cause discomfort?
Build a safe-food foundation: Use foods your child already accepts as a base.
Introduce new foods gradually: Match new foods to the texture, temperature, or colour of their preferred items.
Watch for digestive reactions: Bloating, hyperactivity, or fatigue can reveal intolerances.
Make one small change at a time: Progress is slow, but the payoff is big.
Tips for Making Fruits and Vegetables Easier to Eat
New foods can feel unfamiliar or even overwhelming. The key is to introduce them in ways that feel safe and inviting.
Small changes in flavour, temperature, and pairing can make a big difference.
Use Mild, Familiar Seasonings
A sprinkle of cumin, a dash of cinnamon, or a squeeze of lemon can enhance taste without overpowering. Mild spices make vegetables more flavourful while keeping them easy to accept.
Serve at the Right Temperature
Cold foods may feel refreshing, while warm foods can be more soothing. Some may prefer room temperature for a neutral experience. Experiment to see what works best.
Combine with Preferred Foods
Pairing new fruits or vegetables with a familiar favourite can increase acceptance. Mix finely chopped spinach into dal, blend carrots into dosa batter, or serve cucumbers alongside a favourite dip.
Offer Choices, Not Pressure
Giving options allows more control. Instead of saying, “Eat your carrots,” try, “Would you like roasted carrots or carrot sticks?” The freedom to choose makes mealtimes more comfortable.
Make Eating Visually Interesting
Colours, shapes, and arrangement matter. A fruit salad with vibrant mango and pomegranate may be more appealing than plain apple slices. Fun shapes, like cucumber rounds or star-cut watermelon, can add curiosity and engagement.
What Foods to Avoid with Autism? (Fresh, Clear & Easy-to-Apply Guide)
The gut–brain connection plays a major role in how autistic individuals feel, focus, and respond to sensory input. Certain foods may worsen discomfort, trigger irritability, or intensify sensory overwhelm. That’s why identifying foods to avoid with autism is the first step toward creating calmer mealtimes and better daily balance.
“While some parents report behavioural improvements with gluten-free, casein-free diets, controlled studies have not consistently demonstrated significant benefits. Dietary changes should be approached cautiously and under professional supervision to ensure nutritional adequacy.”
Every autistic individual is unique; what works beautifully for one may not work for another. With that balanced lens, here are the key food categories many families explore and why:
1. Gluten & Casein Sensitivities
Many families try a Gluten-Free Casein-Free (GFCF) diet when digestive issues, bloating, or inflammation seem to worsen behaviour or focus.
Common Gluten Sources
Wheat (atta, maida, bread, roti)
Barley (soups, malt drinks)
Rye (select baked goods)
Common Casein Sources
Milk and milk products
Paneer, cheese, yoghurt
Butter, cream
2. Refined Carbs & Blood Sugar Fluctuations
White bread, sugary snacks, and polished rice can cause rapid blood sugar spikes, leading to irritability, low energy, and difficulty concentrating.
Better Swaps
Brown rice or millet instead of white rice
Whole wheat or gluten-free bread instead of white bread
Dates or fruits instead of packaged sweets
3. Artificial Additives & Preservatives
Packaged foods often contain dyes, flavours, and chemicals that may increase hyperactivity or digestive distress.
Ingredients to Watch Out For
Artificial food dyes (in many candies and snacks)
MSG (in instant noodles, chips, seasoning powders)
Preservatives like nitrates & benzoates
4. Soy & Corn-Based Products
These are common allergens and may cause bloating or discomfort, sometimes even immune reactions.
Hidden Sources:
Soy sauce, tofu, soy milk
Corn syrup in sweets and drinks
Corn starch in sauces, soups, and processed foods
Meal Planning Using an Autism Food List
Once you know what to avoid, planning meals becomes easier, calmer, and more predictable. Here are three simplified meal plans, each crafted for a specific need, sensory ease, gut support, and steady energy.
Meal Plan 1: For Sensory Sensitivities
Soft, neutral-flavoured foods that reduce overwhelm and feel comfortable to chew.
Final Words: Building Peace and Flexibility Around Food
Always remember, mealtime challenges don’t have to turn into battles. Understanding this can help you stay calm and use the coping strategies we discussed earlier to defuse tension.
To get a clearer perspective, introduce new foods alongside familiar favourites and take it slow. Just like we discussed. Involving your child in choosing alternatives and planning “Plan B” options helps build cooperation and flexibility.
Keep trusting the process!
Every small step you take is moving you closer to easier meals and a more peaceful, balanced mealtime for everyone.
For expert insights, support services, and inclusive learning initiatives, visit the India Autism Center.
For parents with children having autism in India, getting an autism disability certificate feels like navigating a maze of forms and hospital visits. Nonetheless, it is one of the most crucial steps in securing essential support and recognition following early detection and diagnosis.
Did you know that in 2021, it was found that about 1 in 127 people have autism? And in India, millions of children are diagnosed with ASD. Many of these children are eligible for government assistance, but only a fraction have an official disability certificate.
So wondering how to get an autism disability certificate in India? We have the answers for you.
Today, we will guide you through everything you need to know, from the process of applying for a disability certificate to obtaining the autism disability certificate in India via the UDID apply portal, including eligibility criteria and required documents, to help and empower autistic individuals.
What Is the UDID, and Why Is It Important?
First things first: what is UDID?
When you asked what UDID is, the answer is that it essentially stands for Unique Disability Identity. It is a national digital initiative by the Department of Empowerment of Persons with Disabilities (DEPwD), under the Ministry of Social Justice & Empowerment, Government of India.
Key highlights of UDID:
A person with a disability can register and apply for a disability certificate on the UDID portal. It is quite simple to apply, track the application status, and request renewals and replacements.
It helps create a centralised national database of PwDs to avoid duplicate entries, making the process transparent and streamlining benefit delivery.
The allotted UDID card will be valid across all the states and union territories in India.
As of 1 June 2021, according to a government notification, certificates issued through the UDID portal are to be the standard across all states/UTs.
How Can UDID Benefit People With Autism?
A UDID card is highly beneficial for children and adults recognised to have autism spectrum disorder (ASD) as per the RPwD Act. Here are the benefits of having a UDID card:
Formal recognition of their disability, which helps in accessing schemes and concessions in education/railways/travel.
Streamlined process (online registration, tracking) rather than wholly paper-based, manual processes.
It becomes easier to present one documented identity for disability status rather than juggling multiple certificates.
So, a UDID card can make the “how to apply for a disability certificate” journey smoother and help to manage an autistic child’s behaviour in a better and more accessible way.
What Is the Eligibility for the Autism Spectrum Disability Certificate?
Under the RPwD Act, autism spectrum disorder (ASD) is one of the 21 specified disabilities. To be eligible for the benefits under the RPwD Act, a person must have a disability of at least 40%, also referred to as the benchmark disability.
Although autism spectrum disorder is included as per the Act, the severity and the functional impact will be assessed medically.
Who Can Apply for Autism Spectrum Disorder?
Before we get into the further details, here is the information that you need to know about who can apply for an autism spectrum disability certificate:
Individuals diagnosed with ASD, or autism spectrum disorder, who are residing in India.
For minors (children), the parent/guardian can apply on behalf of the child.
For adults with ASD, they can apply themselves or via a guardian/representative (if applicable).
The applicant must undergo the prescribed medical/psychological assessment and be recognised by a competent medical board/certification authority.
Some important things to keep in mind:
Diagnosis alone is not enough; the disability certificate must be issued by the competent authority designated under the scheme.
The certificate and UDID card are different but linked; hence, you should apply for both.
The certificate may be for lifetime or temporary validity, depending on whether the disability is progressive or non-progressive.
Step-by-Step Guide: How to Apply for a Disability Certificate & UDID for Autism
The application process for how to apply for a disability certificate for autism can be overwhelming at times. Hence, here are clear steps that can help you understand the procedure, paperwork, and practical tips for smooth processing:
Step 1: Prepare diagnosis, assessment reports, and identity proofs
This step involves collecting all necessary reports and proofs.
Diagnostic report confirming Autism Spectrum Disorder (ASD) from a recognised specialist (paediatrician, psychiatrist, clinical psychologist, or neurologist). The report should be on hospital/clinic letterhead, with signature, registration number, and date.
Functional assessment or developmental assessment results where available (Indian Scale for Assessment of Autism (ISAA), Vineland Social Maturity Scale (VSMS), Childhood Autism Rating Scale (CARS), or equivalent).
Identity & address proof (Aadhaar, passport, voter ID, or other government ID). If Aadhaar is unavailable, another ID can be used.
For a minor, a birth certificate is necessary.
Passport-style photograph (digital upload & physical copy for the board).
Any previous disability certificate or medical records/history (if applicable).
School/therapy reports (for children: special education reports, speech therapy reports). It is a useful form of supporting documentation to demonstrate the functional impact on daily life, schooling, and communication.
Remember:
Ensure that the diagnostic reports are both recent and legible.
If assessments use paper tests, scan and save clear PDFs.
Both physical copies and scanned copies must be kept ready for use.
Step 2: Register on the UDID/Swavlamban portal
Visit the official UDID portal/Swavlamban portal. Look for the section “Apply for Disability Certificate & UDID Card” or “New Enrolment”.
You can register by creating an account (email or mobile OTP verification). Use a parent/guardian’s mobile number or email for child applications.
Fill in personal details accurately: full name, DOB, address, gender, guardian details (for minors), and Aadhaar if available (not strictly mandatory but recommended).
Select the correct disability category and choose Autism Spectrum Disorder (ASD) when prompted.
Upload scanned copies of the photo, identity proof, diagnostic report, and any assessment forms.
Remember:
Save the enrolment/application number shown after submission, as you will need it to track the status.
Some users prefer to save a screenshot of each upload step and the final confirmation page.
Step 3: Fill the form carefully & understand the online vs offline routes
Online process:
The portal typically guides you through the form fields. Common fields: demographic details, disability type, details of the diagnostic centre, uploaded reports, and declaration. Carefully type names exactly as per government ID to avoid mismatch issues at the Medical Board.
Offline process:
If you cannot apply online, many state-level social welfare offices, district disability cells, or government hospitals offer assisted/facilitated enrolment where staff fill the portal entries for you. Keep originals for verification.
Remember:
Mismatch between the name on the Aadhaar and the application, or uploading blurred/partial documents (boards may reject or request resubmission).
Using abbreviations inconsistently, spelling must match across ID/certificate; this inconsistency also needs to be avoided.
Step 4: Attend the Medical Board/Assessment centre (the crucial evaluation)
The board will verify the identity documents and original diagnostic assessments.
They will further perform a functional assessment to estimate how autism affects daily living (communication, social skills, and adaptive behaviour). The medical board for ASD typically includes paediatricians, psychiatrists, clinical psychologists, and/or neurologists, depending on the state and facility.
The board may ask questions to the parent/guardian about milestones, communication, behaviour patterns, school performance, and therapy history.
They may conduct or request additional tests (if the submitted reports are insufficient).
The board will document the percentage of disability (if applicable) and determine whether the person meets the benchmark disability threshold (commonly 40% or higher) for benefits.
Remember:
Carry all originals + 2–3 photocopies of each document (ID, diagnostic report, assessments, school reports).
Please bring any assistive devices you use (e.g., hearing aids or communication devices, if applicable).
For children, bring a familiar toy or comfort item and plan the appointment at a time when the child is calm.
Bring a parent/guardian who knows the child’s developmental history and can answer questions about daily functioning.
Step 5: Certificate issuance, downloading e-certificate & how to get UDID card
Once the board approves, the issuing authority uploads the certificate details to the UDID portal. Now, how to get the UDID card? You will receive an approval notification (via SMS/email) with a link or enrolment reference.
Log in to the portal with the help of your enrolment number and download the disability certificate (often in PDF/e-certificate format).
The portal will also generate the UDID card (unique number and e-card). Many states issue an e-UDID immediately; physical UDID cards are sent later or can be printed locally.
Remember:
Check name spelling, DOB, disability type (Autism/ASD), percentage (if stated), and validity. If anything is incorrect, please raise a correction request immediately via the portal or the relevant issuing authority.
Step 6: Track applications, renewals, updates, and replacements
Here are the steps that you can follow to track the status:
Use the enrolment/application number on the UDID portal to see the status: Submitted → Document Verification → Medical Board Pending → Approved/Rejected.
Some certificates are lifetime, while others (often for children or when a temporary assessment is done) have a validity period (e.g., 3 or 5 years). The certificate will clearly note the validity. Renew your plan at least one month before expiry, if required.
The UDID portal allows users to update their personal details and request a replacement UDID card if it is lost/damaged. Use the “Update” or “Replace UDID” options and follow the verification steps.
Common Mistakes to Avoid
When you are applying for an Autism Disability Certificate or a UDID card, it can feel challenging. The good news? Most delays and rejections occur due to a few simple, avoidable mistakes. Understanding these beforehand can save you weeks of waiting and multiple hospital visits.
Below are the most common mistakes applicants make, along with detailed explanations to help you avoid them completely.
1. Submitting Incomplete or Outdated Medical Reports
Yes, one primary reason why applications get delayed is due to incomplete or outdated medical documentation.
Disability assessment teams require recent, complete, and standardised autism evaluation documents, especially tools such as ISAA (Indian Scale for Assessment of Autism).
Hence, ensure that all the reports are recent and up-to-date.
2. Not Visiting an Authorised Government Hospital
Visiting a private or a non-recognised hospital to get the reports can prove to be a mistake. Only government-certified medical boards are authorised to validate and issue a disability certificate.
Visit only district hospitals, government medical colleges, AIIMS, or state-run disability assessment centres. You can find it via the location tool on the UDID website.
3. Uploading Wrong or Low-Quality Documents
Incorrect file formats or blurry uploads can lead to rejection on the UDID portal. It is necessary to upload a clear and readable document. If it is not clear, it can get flagged by the system immediately.
Make sure that all documents are scanned clearly. Save it as a PDF, JPG, or another format that is within the supported size limit.
4. Missing Signatures or Stamps on Documents
A small detail, but one of the most common reasons for re-evaluation. Remember that unsigned reports are treated as incomplete medical evidence.
Ensure that you check every page for the doctor’s signature & hospital seal, and the assessment report has the official designation of the doctor.
5. Not Providing Correct Guardian/Parent Details (for children)
There can be verification issues if the parent details are mentioned incorrectly. The details must match the information on the Aadhaar card and birth certificate for correct authentication.
It is a best practice to double-check spellings, DOB, and ID numbers. Also, ensure that the parent applying is legally authorised as well.
6. Ignoring the “Permanent Disability” Section
Autism is classified as a lifelong neurodevelopmental condition, but many applicants mistakenly check “temporary disability”. If you select the temporary option, it can trigger yearly renewals and reassessments.
Always select ‘Permanent Disability’ when filling out UDID forms, since autism does not resolve with age.
7. Not Keeping Photocopies of All Submitted Documents
It might not seem important, but it is necessary to keep copies of all the hospital submissions. It will come in handy, especially if the hospital requests a resubmission.
Creating a folder and keeping all documents, along with UDID acknowledgement receipts, stored properly is a wise decision.
8. Delaying Follow-ups After Medical Board Assessment
Once the assessment is done, some applicants forget to track their status online. If any clarification is needed, delays can stretch for months.
Check your application status every 7–10 days on the UDID portal. Also, be sure to respond immediately if the portal indicates a document correction is required.
9. Not Reviewing the UDID Card Details After Issuance
Many people download the card without verifying details such as the disability percentage, name spelling, or date of birth. Any error requires a correction request, which takes additional weeks.
Verify each detail carefully, and if needed, apply for correction within 30 days of issuance.
10. Assuming the Process Is the Same in Every State
Each state has slight differences in hospital listings and scheduling of assessments. It is necessary to verify and follow the most recent guidelines to avoid any errors on your part.
Check your state-specific UDID instructions on the UDID portal for guidance. You should also confirm the hospital’s eligibility beforehand.
Conclusion
The process of obtaining an Autism Disability Certificate and UDID card in India can become easier if you are aware of the steps involved and the documents required, and understand the common mistakes that cause delays. With the right preparation and accurate medical assessments, families can complete the process smoothly and unlock essential benefits, support services, and government schemes that ensure better access and inclusion for individuals with autism.
Frequently Asked Questions
What is an Autism Disability Certificate?
An Autism Disability Certificate is a government-issued document that officially recognises autism as a disability under the RPwD Act, 2016. It helps individuals access support services, education accommodations, financial benefits, and various welfare schemes.
How do I apply for a disability certificate online through the UDID portal?
You can apply by visiting the UDID portal, registering with your details, uploading the required documents, and booking a medical assessment. After approval, the digital UDID card can be downloaded from the portal.
How do I get a UDID card after receiving the disability certificate?
Once the medical board approves your disability, your UDID card is generated automatically. You can log in to the UDID portal, check your status, and download the digital card.
Can private hospital reports be used as part of the application?
Private reports may support the diagnosis, but the final assessment must be done at a government medical board. Only their evaluation is accepted for issuing a certificate.
For expert insights, support services, and inclusive learning initiatives, visit the India Autism Center.
Every parent is eager to hear their child’s first words, regardless of whether it is as simple as “no”. But what happens when those words take longer to come? You might start to wonder: Is my child just a late talker, or could it be something more, like autism?
It is a natural question that comes to mind. Especially when speech delay is a common occurrence in children aged 3 to 5 years. On the other hand, globally, about 0.77% of children are diagnosed with ASD (Autism Spectrum Disorder).
Because both conditions can present as “delayed speech”, it’s easy for parents to feel confused or even alarmed when milestones don’t align.
The good news is that speech delay and autism are not the same. Understanding the subtle yet important differences between the two can help you take the right steps early, whether that means seeking speech therapy, undergoing development, or simply requiring more time and support.
Today, we will explore the speech delay vs autism and discuss what parents and caregivers can do to support individuals with these conditions.
Understanding Speech Delay
In simple terms, speech delay is when a child is unable to produce words or sentences in comparison to other children their age. However, the pattern of learning typically follows a similar path.
Children with speech delay typically understand what’s being said to them (their receptive language) but struggle to express themselves verbally (expressive language).
For example, they may follow instructions such as “Bring your shoes,” but they may not be able to say “shoes here” or even “I want shoes.”
Some of the most common speech delay symptoms include:
Limited babbling by 12 months
No single meaningful words by 16–18 months
Not combining words by age 2 (e.g., “want juice”)
Speech that’s difficult for even the family to understand
Frequent use of gestures to communicate instead of words
There are different reasons that can lead to speech delay, such as hearing impairment, oral-motor difficulties, cognitive delay, multilingual environments, or simply a “late bloomer” tendency.
In conclusion, speech delay does not imply autism.
Understanding Autism Spectrum Disorder (ASD)
Autism, otherwise known as Autism Spectrum Disorder (ASD), is a neurodevelopmental condition which has an effect on communication, social interaction, and behaviour. It is to be noted that speech delay is one of the symptoms of autism, but many more developmental differences define if a child has autism.
Often, children who have autism develop speech delay. Sometimes, a child with autism might not even have a speech delay. However, even when words appear, they may use them in unusual ways (e.g., repeating phrases or scripting lines from TV shows).
Some of the most common autism symptoms include:
Reduced eye contact or social engagement
Limited use of gestures such as pointing towards an object or waving
Lack of response to name
Repetitive behaviours (flapping, lining up toys, spinning objects)
Strong preference for routines or sameness
Sensitivity to sound, touch, or light
Speech that’s monotone, robotic, or echolalic (repetition of words or phrases)
Contrary to popular beliefs, autism does not happen due to poor parenting, vaccination, or poor diet. It is essentially a neurological and developmental issue. If diagnosed early, with proper treatment, communication, and social skills can improve considerably.
Speech Delay vs Autism: Key Differences
It is a natural phenomenon to feel confused between speech delay as well as autism. However, they are different from one another. When a child struggles with forming or using words, it is a speech delay, while autism involves broader challenges in communication, social interaction, and behaviour.
It is essential to understand the distinction between speech delay and autism, allowing for timely intervention. Here is a side-by-side comparison of speech delay vs autism:
Feature
Speech Delay
Autism
Primary issue
Slower speech development; articulation or word-use lags
Core issues in social communication & interaction + repetitive behaviours; speech may be delayed or atypical
Social engagement
The child typically uses gestures, points, makes eye contact, and tries to communicate non-verbally despite delayed speech.
The child may have reduced eye contact, limited pointing or gesturing, less joint attention and may prefer solitary play.
Non-speech behaviours
Usually no major behavioural or play issues beyond the speech domain.
Presence of repetitive behaviours, restricted interests, difficulty with change of routine, etc.
Outcome & intervention
With speech therapy and support, many children catch up.
Lifelong profile; early intervention helps significantly, but the condition tends to remain on the spectrum.
Speech pattern
Typical pattern but slower; errors in production, short phrases.
Speech may be absent/very delayed or present but atypical (echolalia, literal language, unusual prosody).
For example, when a two-year-old doesn’t speak but points to objects, imitates gestures, and also plays pretend, speech delay may develop. On the other hand, a child who does not point to any object, tends to avoid eye contact, and often fixates on spinning objects has higher chances of being diagnosed with autism.
Is Speech Delay Autism?
Since it is easy to get confused due to similar symptoms of both speech delay and autism, the reality is that speech delay itself is not autism. However, one of the many symptoms of autism is speech delay when it appears along with social as well as behavioural differences.
Many children with speech delays do not have autism and catch up with therapy, but if other developmental red flags appear, further assessment is needed.
So, is speech delay autism? No, a child with speech delay is not autistic, but every child with autism tends to have speech delay.
Signs that Hint at Autism in the Presence of Speech Delay
Speech delay is an early sign of autism. However, it is not necessarily always the case. Hence, it is essential to recognise the additional signs to look for. Here are some “red flag” behaviours:
If you find that there is limited babbling by 12 months. Or if there is a loss of babbling.
No single words by 16 months, or loss of previously acquired words.
Not pointing at objects, not waving or using gestures to display their interest.
Doesn’t respond to their name by 9-12 months or seems indifferent.
Limited eye contact or social smiling.
Often displays repetitive behaviour, mainly including hand-flapping, spinning objects, or even lining up their toys.
Strong preference for sameness and difficulty with change.
Unusual speech: echolalia, literal language, or monotone or robotic prosody.
If many of the listed signs begin to appear, it is time to have a complete evaluation done.
Why Does Making the Distinction Matter?
Understanding whether a child has a speech delay or autism is not about labelling them; it is about finding the right approach to obtain help at the right time. Early and accurate identification allows parents, therapists, and educators to tailor interventions that match the child’s specific needs.
When parents and caregivers understand the difference between speech delay and autism, they can take action and offer support that can have a lifelong impact.
Here is why it is necessary to understand the speech delay vs. autism concepts:
Intervention Timing
Children with speech delays can receive speech-language therapy that can lead to significant catch-up. For autism, early multi-modal intervention (speech, occupational therapy, and behavioural therapy) is linked to better outcomes.
Focused Therapy
For speech delay, focused therapy can be provided to address articulation, sentence formulation, and vocabulary. On the other hand, for autism, more focus is on improving social skills, play skills, sensory regulation, and routine management.
Expectations and Support Services
Families of a child who is diagnosed with autism may have the chance to access specialised services, support networks and long-term planning. Appropriate planning can only be done when a parent understands the distinction between speech delay and autism.
Monitoring and Collaboration
If you treat it as a speech delay but miss warning signs of autism, you might miss an earlier chance to intervene more comprehensively.
What Can Parents and Caregivers Do?
Parents and caregivers have to be aware of communication delays, as they can be both confusing and emotionally distressing. The key is not to panic but to take proactive, informed steps.
There are different steps that parents as well as caregivers have to take, such as seeking a professional evaluation, engaging in early intervention programmes, or using supportive communication techniques at home. It can make a significant difference.
The measures that a parent or a caregiver can take include:
1. Tracking Development Milestones
You can utilise speech or language milestones such as babbling by ~9–12 months, single words by ~16 months, and two-word phrases by ~24 months. If your child is not meeting expected milestones, it is essential to consult a paediatrician, a developmental paediatrician, or a speech-language pathologist.
Reaching out to a professional can help you determine if the issue is just related to speech delay or if other broader developmental or behavioural signs imply autism.
2. Engage in Early Intervention Services
Once you have a diagnosis or developmental report, don’t delay intervention. In India, early intervention programs, such as speech therapy, occupational therapy, and behavioural therapy (like ABA).
These therapies help to improve communication, cognitive development, and social interaction skills. The earlier the therapy begins, the more effective it tends to be.
3. Practise Speech and Communication at Home
Parents have to include interactive activities in their child’s speech development to enhance their child’s speech skills. Here are some actions that can help:
Reading storybooks aloud every single day
Naming different objects while playing
Encouraging to repeat simple words
Singing rhymes or using picture cards
It will strengthen both expressive and receptive language and also create a positive communication environment.
4. Observe and Encourage Social Interaction
Social reciprocity is a common challenge that children with autism face. Some symptoms include difficulty making eye contact, difficulty sharing joy, and not responding to their name when called.
It is essential to foster small but meaningful interactions through play-based learning, where communication occurs naturally and organically. You can encourage children to get engaged in playing turn-based games or engage in pretend play, which helps build joint attention and empathy.
5. Stay Patient and Consistent
Parents/caregivers need to understand that progress will not happen overnight. Whether your child is receiving speech therapy or autism support, consistency and emotional reassurance matter most.
It is important to celebrate even minor milestones. Moreover, a calm environment is to be maintained. It also helps to keep routines predictable, as it provides a sense of safety for children with communication difficulties.
6. Join Support Networks and Communities
Parents who have children with such concerns can feel quite calm yet empowered when they connect to other parents with similar experiences. You’ll gain practical tips, emotional support, and access to professionals who specialise in both speech delay as well as autism management.
How Does Therapy Differ for Speech Delay vs. Autism?
Even though certain symptoms are similar for speech delay and autism, the treatment approaches for speech delay versus autism are quite different. Understanding these distinctions helps parents choose the right kind of intervention tailored to their child’s unique developmental needs.
Here is a side-by-side comparison of how therapy differs for speech delay versus autism:
Therapy Focus
Speech Delay
Reading aloud, naming objects, and interactive play
Main Goal
Improve articulation, vocabulary, and sentence use
Enhance communication, social understanding, and behavioural regulation
Visual schedules, sensory integration, and structured social activities
Visual schedules, sensory integration, structured social activities
Expected Outcome
Catching up to peers within 6–12 months of therapy
Gradual progress; lifelong communication growth with continuous support
When to Seek Professional Help?
Do not wait for the condition to get worse. Once you find the signs below, it is time to seek professional help:
Isn’t babbling by 12 months
Doesn’t say single words by 16–18 months
Doesn’t combine words by 24 months
Doesn’t respond to their name or show interest in people
Avoids eye contact or play interaction
You can consult a speech-language pathologist or a developmental paediatrician. If you get early screening for your child, it can help in better identification.
Conclusion
Whether it is speech delay or autism, it can tend to confuse parents and make them concerned, as the symptoms overlap. A speech delay mainly has an effect on a child’s ability to use or understand language, while autism involves broader challenges in communication, behaviour, and social connection. Identifying the distinction will help the child receive the right help.
With actions including early detection, consistent therapy, and compassionate guidance, children with communication challenges can make remarkable progress. Ultimately, it is essential to recognise that each child is unique and develops at their own pace.
Frequently Asked Questions
Is speech delay the same as autism?
No, they are not the same. Speech delay affects a child’s ability to produce or use words, while autism (ASD) involves challenges in social communication, sensory processing, and behaviour. Some children with autism may have speech delays, but not all children with speech delays have autism.
What are the common symptoms of speech delay?
Typical speech delay symptoms include limited vocabulary for age, unclear speech, difficulty forming sentences, and frustration when trying to communicate. However, these children typically show an interest in interacting with and understanding others.
What causes speech delay?
Speech delay can result from hearing loss, oral motor issues, bilingual exposure, lack of stimulation, or neurological conditions. It doesn’t necessarily indicate autism, but it may need professional assessment to identify the cause.
How is autism diagnosed?
To diagnose autism, developmental assessments, observing the child’s behaviour, and standardised tools like the ADOS (Autism Diagnostic Observation Schedule) are used.
For expert insights, support services, and inclusive learning initiatives, visit the India Autism Center.
Coping with autism can feel like a sudden shift in gravity. Relief and grief, clarity and confusion, all crowd in at once. There is the label (with that comes the stigma), the paperwork, and the inevitable questions.
And then the quiet pause of “Now what?”
Long before that moment, though, many live through a drawn-out pre-diagnosis phase. Includes studying, noting patterns, and preparing questions for the consultant. These steps, modest as they seem, help steady the ground and make the conversation ahead more coherent.
Our guide on coping with autism diagnosis is meant as a compass through both stages—the groundwork before diagnosis and the path that unfolds after. Up next, we’ll break down what the diagnosis truly means and how to cope with autism in daily life.
Read on.
Coping with Autism Diagnosis: What It Means
You’ve heard the word. You’ve sat through the explanation.
Now you’re holding a diagnosis that’s supposed to help, but doesn’t quite tell you how. Even with a name, coping with autism spectrum disorder is rarely straightforward – it often opens a new set of questions you didn’t know you’d be asking.
Pam Aculey, parent of a child on the spectrum, says, “Receiving our son’s autism diagnosis was a life-changing moment. Whilst it provided us with an explanation… it also instilled panic, confusion and uncertainty for the road ahead.”
That mix of clarity and overwhelm is something many families feel in the days that follow. Understanding the different diagnostic labels is the first step in finding autism coping skills that actually fit.
Your child meets the criteria for Autism Spectrum Disorder, Level 2
This statement reflects the current diagnostic model under the DSM-5, where autism is recognized as a spectrum rather than distinct subtypes like Asperger’s or PDD-NOS.
Level 2 suggests substantial support needs, especially in areas like social interaction, communication, behavioral flexibility, and sensory regulation.
You may notice:
Frequent meltdowns when routines change
Limited back-and-forth interaction
Delayed speech or unusual language patterns
High sensitivity to noise, touch, or crowds
What this might mean:
Referrals for speech therapy, occupational therapy, and behavior-based interventions
Likely need for a special educator or shadow teacher in inclusive settings
Monthly therapy expenses in private setups can run ₹15,000–₹30,000+
Eligible for disability certification under the RPwD Act, which can support access to schools, concessions, and future government schemes
Often, children at this level may also be evaluated for co-occurring conditions like ADHD, sensory processing difficulties, or speech apraxia. Each of these can shape therapy goals and timelines. Families often ask how to cope with autism when support needs are substantial. At this level, coping strategies for autism usually include speech therapy, occupational therapy, structured routines, and professional guidance.
Traits consistent with autism, Level 1
Level 1 autism indicates milder but still impactful support needs. Individuals may have fluent language and average cognitive abilities, but experience difficulty with social nuance, rigidity, anxiety, or sensory overload. These are often internal struggles that others don’t easily see.
This is where high functioning autism coping strategies often come into play – building social confidence, coaching for executive skills, and offering tailored counseling.
What this might mean:
May go unnoticed in school unless academic or emotional challenges appear
Needs may include counseling, executive function coaching, or group therapy
Girls and verbally articulate children may mask symptoms, leading to delayed or missed diagnosis
Support may feel optional to others, but burnout and withdrawal are real risks
Financially, it often means unstructured, ongoing out-of-pocket expenses for private support with little formal recognition
Diagnosis at this level may be made later in life, especially in women, nonbinary individuals, or those misdiagnosed with anxiety, OCD, or depression. For adults, it can feel like both clarity and reckoning.
ADHD and autistic features are both present
This is a dual diagnosis that’s becoming more widely recognized. ADHD and autism often overlap, with each condition amplifying the other’s challenges. A child might struggle to sit still and also resist transitions. An adult might be impulsive, yet hyper-focused and anxious in new social situations.
What this might mean:
Need for a combined intervention plan: behavioral therapy, sensory tools, and classroom strategies
In some cases, medication may be advised to manage inattention or hyperactivity
School systems may struggle to support both diagnoses simultaneously
Costs can quickly add up—between therapy, psychiatric consults, and parental guidance
Most insurance plans don’t fully cover these needs in India
Clinicians often highlight this combination to explain why a child doesn’t respond to a single therapy style—or why social skills improve, but regulation doesn’t.
Parents may need to explore combined coping mechanisms for autism and ADHD, including behavioral therapy and school accommodations.
Social Pragmatic Communication Disorder fits better
This diagnosis is given when social interaction is affected—like difficulty understanding tone, taking turns in conversation, or interpreting gestures—but without the repetitive behaviors or sensory differences seen in autism.
It’s considered distinct from ASD, but support is still essential. What this might mean:
May be referred to speech-language therapy focused on social communication
Often excluded from autism-specific school accommodations and benefits
Teachers may misread challenges as immaturity or rudeness
Parents sometimes ask how they’re supposed to hold it all together. The answer isn’t about perfection so much as steadiness.
Your own regulation is the anchor. If you can stay steady, you’ll catch the small signs of frustration and step in before it tips into a breakdown. Every problem cannot be immediately fixed but just staying watchful will help you detect if your child is getting pushed over the edge, and you can check that in time!
Puja Dutta, RCI-registered Clinical Psychologist at India Autism Center
Long-term support is still needed, but legal protections and public funding are limited. This diagnosis can feel ambiguous for parents, but the key is not waiting. Social communication skills can improve dramatically with early, targeted support.
Even without a full autism diagnosis, families benefit from autism coping skills for adults and children alike – skills like emotional regulation, communication strategies, and sensory support.
Developmental delay with autistic features; we’ll reassess
Used for children under 5 when delays are observed across areas—like speech, motor skills, or play—but a full autism diagnosis is not yet confirmed. It’s a watch-and-intervene approach.
This overlaps with Global Developmental Delay (GDD), a term that gives space to monitor evolving needs.
What this might mean:
Begin early intervention immediately: speech, OT, special education
Track milestones closely, with reassessments every 6–12 months
May receive temporary disability certification to access early support
Therapy costs are often high upfront, with limited public provision
Diagnosis may later evolve into ASD, ID, or a learning disability, depending on the child’s developmental path
Early intervention here focuses less on labels and more on developing autism coping skills – speech, play-based learning, and structured support routines.
So, now that you’ve unpacked the language, let’s move toward what to actually do with it. Next up: building a plan, finding the right support, and making this diagnosis work for you.
Personalizing Support: What to Focus on, What to Let Go
Parents of autistic children are often handed a flood of advice. New therapies, new strategies, new “essentials.” What gets lost in that rush is a quieter truth: not every approach matters equally. What matters most is finding coping strategies for autism that fit the child in front of you.
Support becomes clearer when you slow down long enough to notice. Which moments seem to calm? Which spark tension? Which gestures or sounds carry meaning? A pattern begins to reveal itself, and with it, the outline of a plan.
Seen this way, the next steps become clear.
Decode Sensory Clues Before Labeling Behavior
A child covering their ears in a crowded room is not being difficult; they are signaling distress. A refusal to wear a certain shirt may point less to stubbornness than to the irritation of a seam. Behavior, in this sense, is language—sometimes subtle, often urgent.
Check these common sensory signals found in autism and ways to respond:
If You Notice This
It May Reflect
You Can Try
Hands clamped over ears
Auditory sensitivity
Noise-canceling headphones, quiet breaks
Refusal of clothes/shoes
Tactile discomfort
Softer fabrics, tagless clothing
Chewing on sleeves or pencils
Oral sensory-seeking
Chewelry, crunchy snacks
Pacing, spinning, or jumping
Need for movement
Swings, trampolines, and climbing breaks
Withdrawal in bright rooms
Visual overload
Dim lighting, sunglasses
When interpreted this way, behavior shifts from being a problem to be managed to a clue about how the world is being experienced.
This forms part of everyday coping mechanisms for autism, helping children regulate without escalating stress.
Use Routine to Create Safety, Not Rigidity
Routines are often described as restrictive, but for many autistic children, they serve as anchors. Predictability eases anxiety, creates a sense of safety, and makes daily life less chaotic. The goal is not rigid adherence to schedules but a rhythm steady enough to provide reassurance.
Ways routines can ease daily life:
Goal
Tool That Helps
Calmer mornings
Picture strip by the mirror
Smoother bedtimes
Dimmer switch + checklist
Easier transitions
Countdown timer + verbal cue
Less chaotic weekends
“Today’s Plan” fridge chart
Sometimes the most effective support is not a full overhaul but a small, consistent addition that lowers stress.
For many families learning how to live with autism, routines become a key autism coping skill that provides both safety and flexibility.
Expand Communication Beyond Speech
Spoken words often arrive unevenly, or not at all. Yet communication rarely disappears. It shows up in gestures, repeated phrases, the rhythm of movement, or with the help of assistive devices. To recognize those signals is to widen the frame of what language looks like.
Ways to make communication more accessible:
Offer clear picture choices instead of open-ended questions
Treat repeated scripts as openings, not interruptions
Allow extra pauses before stepping in
Keep AAC tools close during everyday routines
By shifting attention from what is absent to what is present, communication begins to feel broader, more possible.
Communication supports are essential coping skills for autism spectrum disorder, especially when speech is delayed or absent.
Teach Regulation Before the Storm
Meltdowns rarely arrive without warning. They build gradually—restlessness, escalating scripts, withdrawal. These are not minor inconveniences but early signals that the child is nearing a breaking point. Intervening before escalation often means the difference between a spiral and a moment of calm.
Here are some early clues and supports that prove useful:
Early Clue
Helpful Support
Pacing or restless hands
Fidget tools, deep pressure
Escalating scripts
Calm break, quiet corner
Covering ears or eyes
Headphones, dim lights
Repeated questions
Visual schedule, consistent reply
Calm practices introduced early and often, not in the midst of a crisis, are the ones most likely to take hold. These proactive methods are some of the most reliable autism coping skills for adults and children.
Start With Strengths, Not Deficits
The impulse to focus on delays is strong, but strengths are often the more reliable path forward. A child’s fascinations, talents, or even quirks can become tools for learning and connection. What lights them up can also guide them toward growth.
Transform strengths into supports:
Strength
How to Build On It
Fascination with trains
Counting, turn-taking, sequencing
Love of drawing
Self-made visual schedules
Strong memory for patterns
Anchoring routines and rules
Mimicry of sounds
Social scripts and play
Passion for animals
Responsibility and empathy-building
When growth is anchored in strength, progress often feels less like correction and more like expansion. This strength-based model not only builds skills but also teaches coping strategies for autism by creating positive learning anchors.
Support, then, is not about adding more. It is about finding the shape that matches a child’s needs and leaning into it. Observed closely, the outline is already there.
Use Cognitive Training to Strengthen Core Skills
In India, cognitive training is slowly gaining traction as an essential part of intervention for children with developmental differences. Unlike therapies that target specific behaviors, cognitive training strengthens the “thinking skills” beneath them with flexibility, self-regulation, multitasking, working memory, and problem-solving. These are the foundations that help a child adapt in the classroom, manage frustration, and carry new learning into daily life.
Why it matters: Without these skills, even strong abilities, like language or memory, may not translate into independence. A child who can memorize facts may still struggle to shift when plans change; one who speaks fluently may still be derailed by poor regulation. Cognitive training fills these gaps by teaching children how to manage information, not just absorb it.
For many, especially when coping with ASD as an adult, cognitive training becomes a crucial tool for independence and daily functioning.
What it looks like:
Memory and sequencing games to strengthen working memory
Structured play that encourages flexible thinking
Daily activities that demand planning and self-monitoring
Looking Ahead: Financial Foundations for Lifelong Support
Financial planning becomes essential once an autism diagnosis enters a family’s life. It is the start of a long journey to ensure your child’s needs are met today and protected for tomorrow. A strong financial plan is just as vital as therapies and coping skills for autism. It ensures that support systems continue long-term, especially as children transition into adulthood.
In India, families can explore government-supported Niramaya Health Insurance, covering hospitalization and therapy, or private options like Star Special Care, which includes medical, therapy, and hospital expenses. Internationally, programs such as UnitedHealthcare Special Needs Plans or AXA disability coverage offer comprehensive long-term support. These plans do more than pay bills. They create a safety net that lets daily life unfold with less uncertainty.
A thoughtful financial strategy brings calm and confidence. Planning early safeguards not just care, but your child’s dignity and future possibilities. If you’re unsure which options fit best, a consultation with a specialist can help map the path forward.
Frequently Asked Questions
Coping skills are strategies that help manage sensory sensitivities, emotional regulation, and social interactions. They can include routines, mindfulness exercises, sensory tools, and structured problem-solving approaches.
Autistic individuals use a mix of self-developed routines, environmental adjustments, and support networks. Some rely on structured schedules, hobbies, or technology, while others use therapy-informed strategies to navigate social or sensory challenges.
Yes – autism does not preclude a fulfilling, independent life. “Normal” is relative, but with support, skills development, and accommodations, autistic people pursue education, careers, relationships, and hobbies like anyone else.
Adult coping often focuses on self-advocacy, emotional regulation, and building sustainable routines. Leveraging therapy, peer support, workplace accommodations, and personal strengths helps navigate daily demands and life transitions effectively.
Coping with autism as a parent involves balancing emotional support, structured routines, and consistent therapy for your child. Understanding your child’s sensory cues, building communication strategies, and seeking support networks can make daily life smoother.
Effective coping strategies include maintaining predictable routines, using visual schedules, leveraging cognitive training, and focusing on your child’s strengths. Behavioral therapy, speech and occupational therapy, and family counseling also play a vital role. For more personalized coping strategies for autism, you can reach out to the experts at IAC. Contact us for guidance.
Nonverbal children can often communicate through gestures, picture cards, AAC tools, or repetitive scripts. Recognizing these signals as language and encouraging alternative communication methods is essential.
Resources include early intervention centers, speech and occupational therapy services, special educators, and government programs like disability certification under the RPwD Act. Private insurance options like Niramaya Health Insurance or Star Special Care can help manage therapy costs. For a personalized roadmap to these resources, reach out to IAC.
Yes! Adults on the autism spectrum can develop coping skills through cognitive training, social skills coaching, and structured routines. Learning self-regulation, mindfulness, and stress management strategies can significantly improve quality of life.
For many parents with autistic children, the first worry begins with silence. A toddler who doesn’t say “mama” at 18 months. A child who once spoke but then suddenly stops.
Speech development and the question ofwhat age do kids with autism start talking is not one-size-fits-all journey. Research even shows that about 25–30% of children with autism remain minimally verbal beyond the age of five.
These wide variations can feel confusing and even frightening for families. But understanding the signs your autistic child will talk can replace fear with clarity.
So, in this article, we’ll explore at what age do autistic children talk, why timelines differ, and what signs may suggest your child will eventually find their voice.
At What Age Do Kids with Autism Start Talking? Speech Development Timelines in Autism
In typical development, speech moves from babbling to first words, short phrases, and then full sentences.
In autism, these stages may appear later, occur out of order, or look different. Sometimes, there are repeated phrases from others, or long stretches of silence followed by sudden bursts of speech. Parents often ask: “When do autistic kids start talking?” The truth is, the answer varies for each child.
Here’s how typical timelines compare with those on the spectrum:
Cooing and Babbling (2–6 months)
For most infants, the soundtrack of early life begins with rounded vowels like “oo” or “ah”. These soon sharpen into rhythmic “ba-ba” and “ma-ma.”
In autism, these sounds may come later, occur less often, or take different forms such as humming, squealing, or repetitive tones. Sometimes, words appear suddenly and then vanish, leaving parents wondering: “When did your autistic child start talking?”
First Words (12–18 months)
By around 12 to 18 months, children typically begin speaking their first intentional words. Simple ones like “mama” or “ball,” used with meaning.
In autism, however, first words may be delayed beyond age two, appear briefly before fading, or emerge inconsistently. This often leads to the question: “Will my autistic son ever talk?”
As Puja Dutta, RCI-registered clinical psychologist at the India Autism Center, explains,
Between the ages of 14 months to 2 years, some parents report that the child was developing normal speech milestones and then, either abruptly or within a short span, a regression in speech is noticed.
Two-Word Phrases (18–24 months)
The leap from words to short phrases, like “want juice” or “go park,” marks a milestone in combining meaning.
In autism, this step may be postponed or shaped by echolalia, the repetition of words and phrases borrowed from others, before original pairings begin to emerge.
Simple Sentences (2–3 years)
Most children now form 3–4 word sentences such as “I want toy” or “Go see dog.”
In autism, sentence-building tends to be slower, often anchored in concrete language, with abstract or flexible use of words taking longer.
Conversational Skills (3–5 years)
By preschool, most children can trade questions and answers, shift tone to suit the moment, and navigate the give-and-take of talk.
Autistic children may command a wide vocabulary yet struggle with pragmatics. It’s the unspoken rules and rhythms of conversation that are more elusive to them. Parents often ask: “Do non verbal autistic kids ever talk?” The answer: yes, many do, but at their own pace.
Verbal and Non-Verbal Development in Autism
Unlike typical language growth, which follows a fairly predictable path, speech and language development in autism is often uneven. Some individuals on the spectrum speak fluently, while others use only a few words.
At the same time, this raises another concern: “Do nonverbal autistic children ever speak?” Research and therapy show that yes, many may rely on gestures or augmentative and alternative communication (AAC) devices.
Here’s how different communication profiles typically present:
Profile
Key Characteristics
Common Challenges
Primary Communication Methods
Verbal Autism
Spoken words or sentences; may include echolalia, unusual prosody, or highly specific vocabulary
Conversational reciprocity; adapting language to context; interpreting tone and social cues
Spoken language, sometimes supported by visual aids or AAC
Non-Verbal / Minimally Verbal Autism
Few or no spoken words; may have strong receptive language skills
Initiating speech; sustaining verbal interaction
Gestures, facial expressions, sounds, AAC such as picture boards or speech-generating devices
In practice, autistic individuals often blend verbal and non-verbal methods depending on the situation. Communication is fluid, not fixed, and the most effective approach is one that adapts to each individual’s strengths.
Signs Your Autistic Child May Begin Talking Soon
Early signs of language growth aren’t always about words. They can emerge in tone, rhythm, gesture, or shared engagement. Parents often search for clues about when do kids with autism start talking.
Here are some ways your child may show that speech is beginning to take shape:
Your child imitates sounds and actions
Clapping when you clap, humming back a tune, or trying a new consonant sound. All of these show that they’re linking movement, sound, and meaning, laying the groundwork for speech.
Your child experiments with babbling and first words
Playful strings of consonants (“ba-ba,” “ma-ma”) or sporadic single words show that vocal exploration is underway. Speech may come with quirks such as pronoun reversals (“You want cookie” instead of “I want cookie”) or unusual sentence structures. These aren’t errors. They’re milestones in learning how to use language.
Your child uses communicative gestures
Pointing, waving, reaching out, or clapping serve as intentional signals. These gestures bridge the gap between non-verbal interaction and spoken communication.
Your child repeats words or phrases
Children may echo what they hear immediately or repeat it later in a new context. What looks like parroting is actually practice. A way to explore rhythm, self-soothe, or begin forming speech patterns.
Your child engages in pretend play and turn-taking
Tea parties, role-plays, or simple back-and-forth games show your child understands shared narratives. These interactive abilities often emerge alongside language growth.
Your child responds consistently to their name
Turning toward you when called reflects growing social awareness and readiness to connect verbal cues with action.
Your child takes part in back-and-forth exchanges
Whether trading facial expressions, gestures, or playful sounds, these mini conversations mirror the give-and-take of spoken dialogue.
Your child follows a unique path to language
Some children may skip traditional steps. They move straight from silence to whole words, or begin with short phrases before single words. Different doesn’t mean delayed; it’s simply a different path.
Your child’s speech has distinct vocal qualities
Early speech may carry unusual pitch, rhythm, or inflection. While it can sound atypical, it signals that your child is actively experimenting with the mechanics of speech.
Your child shares joint attention
Looking between a toy and you, or drawing your gaze toward an object, reflects the ability to connect experiences with another person. This is one of the strongest predictors of language growth.
Non-verbalism in Autism vs Non-verbal Learning Disorder (NVLD)
Non-Verbal Learning Disorder can be confusing at first glance. Despite the name, children with NVLD often have plenty of words. Sometimes more than expected for their age.
What’s missing is not speech itself, but the other half of communication. The unspoken layer.
The glance that signals understanding, the pause before answering, the change in tone that shifts a conversation. These subtle cues can slip past unnoticed.
In autism, “non-verbal” tends to mean something quite different.
Speech may be limited, inconsistent, or absent altogether. Communication often shows up through gestures, body language, scripted phrases, or assistive devices. The social frame is present, but the words themselves may take longer or follow an unexpected path to arrive.
Both NVLD and autism reshape how communication unfolds. NVLD leaves the sentences intact but makes the social context harder to grasp. Autism preserves the context but may set words further away.
Sometimes present, sometimes not; may use devices, gestures, or signs
Fluent, often early; vocabulary usually strong
Main challenge
Expressing thoughts and needs when speech is unreliable
Reading the silent language of social interaction
In conversation
May avoid verbal back-and-forth or speak in a distinct rhythm
May speak at length but miss the subtle social undercurrents
Underlying difference
How language, sensory input, and social cues connect
How the brain interprets space, patterns, and non-verbal signals
Early years
Fewer early words, less babbling, more pointing or gestures
Strong with words, but interpreting social cues, puzzles, or spatial tasks can be difficult
How Speech Therapy Can Support Your Non-verbal Child
For many parents, the hope begins with a single word. The dream of hearing “mama” or “baba” feels both urgent and fragile. When that word doesn’t come, or when it fades away, the instinct is to look toward speech therapy as the magic key.
But here’s the truth: speech therapy isn’t just about getting kids to talk. For non-verbal or minimally verbal autistic children, it’s about finding their language, whether through pictures, signs, devices, or movement, and building on it. Families often ask: “Do nonverbal autistic children ever speak?” Yes, many do with the right support.
That’s why modern speech therapy rarely looks like a child sitting at a desk repeating words. It’s individualized, layered, and often creative.
A few of the most effective approaches include:
Augmentative and Alternative Communication: AAC tools ranging from picture boards to high-tech devices that generate speech.
Picture Exchange Communication System (PECS): A step-by-step program where children learn to exchange images for what they want, laying the foundation for symbolic language.
Total Communication Approach: Using speech, sign language, gestures, and AAC together—so no door to communication stays closed.
Prompts for Restructuring Oral Muscular Phonetic Targets (PROMPT) Therapy: A tactile method where therapists use touch cues on the child’s face to guide speech movements.
Oral-Motor Therapy: Strengthening and coordinating muscles needed for speech, especially when motor planning challenges are present.
Naturalistic Developmental Behavioral Interventions (NDBI): Embedding communication practice into play and routines, making learning part of daily life.
Vocal Play and Shaping: Moving from hums and sounds toward syllables and words, often supported with visual or tactile prompts.
Joint Attention Interventions: Building the foundation of language by helping the child share focus with another person.
Therapy can take place one-on-one, in group sessions, at home with caregiver coaching, or even online. What matters most is that it meets the child where they are, and empowers families to recognize every sound, gesture, or picture as a step toward connection.
Home Speech Intervention Strategies
Speech therapy may happen in a clinic, but the real magic unfolds in kitchens, living rooms, and playgrounds. Everyday routines, the breakfast table, bath time, or a game in the park, are where language comes alive.
The principle is simple: when a child makes an attempt and someone notices and responds, they learn that communication works. That lesson, repeated hundreds of times in small ways, is what builds speech.
Here are some strategies, backed by decades of speech-language research, that parents can weave into daily life:
Model Functional Language: Use short, clear phrases like “more juice” or “open door.” Repeat them in context so the link between words and actions becomes obvious.
Create Communication Temptations: Place a toy just out of reach, or keep the lid on a snack jar. These small obstacles encourage your child to signal for help.
Narrate Actions (Parallel Talk and Self-Talk): Describe what your child is doing (“rolling ball”) or what you’re doing (“pouring water”). It builds a running language map of the world.
Expand and Extend: If your child says “car,” you might add “big car” or “red car.” This gently models more complex language without pressure.
Use Wait Time: After asking a question or making a comment, pause for a few seconds. That extra space gives your child time to process and respond.
Respond to Every Modality: Whether your child points, vocalizes, signs, or uses AAC, treat it as valid communication.
Let Communication Have Consequences: If they ask for water (in any form), make sure they get water. That link reinforces the purpose of communication.
One of the most powerful ingredients here is co-attention. It refers to sharing focus on the same object or activity.
Looking at a drawing together, pointing at a toy, or saying, “Wow, you built this tower!” creates a moment of connection. These small exchanges spark curiosity and open the door to new words.
Important:Skipping therapist-guided exercises, routines, or prompts may feel small in the moment, but over time, it slows or blocks your child’s gains. Every repetition counts.
Parting Words: Beyond Speech Alone
It’s important to remember that when do autistic kids start talking is only part of the story. Some children may never speak fluently, but still develop meaningful communication through AAC, gestures, or devices. Timing, coordination, and repeated practice all play a role.
For some autistic children, additional challenges like dyspraxia or childhood apraxia of speech make producing spoken language even harder.
This doesn’t mean they cannot connect with others. It simply means their journey to verbal communication may take a different path.
When families and therapists recognize these overlaps, the focus shifts from forcing words to opening multiple avenues for communication.
There’s no fixed formula. However, some signs suggest potential for speech development:
Does the child use gestures (like pointing or waving)?
Do they make meaningful sounds, even if not full words?
Do they show understanding—like responding to their name or following simple instructions?
Are they interested in social interaction or imitating sounds/actions?
These are often encouraging signs. Still, some children may use AAC (Augmentative and Alternative Communication) methods instead of spoken words, and that’s equally valid communication.
At what age do autistic children talk?
It varies a lot. Some autistic children speak on time (around 12–18 months), others may start talking at 2, 3, or even after 5 years old.
Some begin with single words, then gradually combine them. Others may have a speech burst later, especially after starting targeted support like speech therapy or play-based interaction.
Do autistic kids talk eventually?
Many do. But not all. Some become fluent speakers, some develop a few functional words or phrases, and others use nonverbal methods long-term.
It’s also common for speech to start and then pause or plateau. This doesn’t always mean it’s lost for good. With the right supports, gains can return or accelerate.
When do autistic kids start talking fluently?
For those who do become fluent speakers, fluency often emerges between 4 and 7 years, sometimes later.
“Fluent” can look different, too: for some, it means full conversations; for others, scripted or echolalic speech may still serve real communication purposes.
Important: Fluency doesn’t always mean social ease. Even verbally fluent autistic individuals might struggle with back-and-forth conversation or emotional expression.
When do autistic kids start talking?
Some start with first words as early as 12 to 24 months, but it’s also common for speech to emerge later, 3, 4, or even 5+ years.
Others may show early speech that regresses or disappears around age 2, especially in children with co-occurring conditions like childhood apraxia of speech.
Do non-verbal autistic kids ever talk?
Yes, some do. “Non-verbal” doesn’t mean “never verbal.”
Many children once considered non-verbal go on to use spoken words—sometimes after age 5 or even 8—especially with AAC support, language-rich environments, and personalized therapy.
Still, some individuals remain non-speaking lifelong, and may thrive using sign language, picture systems, or speech-generating devices.
At what age does an autistic child speak fluently?
If they develop fluent speech, it’s typically around 4 to 7 years old. But this varies. Children who speak early might still struggle with conversational fluency or social use of language well into adolescence.
Others may speak fluently in a structured or academic setting, but not in daily social interactions. That’s still valid communication – just with a different style.
When did your autistic child start talking compared to others?
Parents often share very different timelines. Some report their child said first words around age 2, while others mention speech emerging much later, sometimes after 5 years. This variation is normal, and comparing one child’s journey with another’s can cause unnecessary worry.
Do nonverbal autistic children ever speak later in life?
Yes, some do. Even if a child is nonverbal at age 4 or 5, progress can still happen with therapy, AAC devices, and consistent support. Some individuals develop speech in adolescence or adulthood, though others may prefer nonverbal communication.
What therapies help if my autistic child is not talking yet?
Speech therapy, AAC tools, and naturalistic play-based approaches are widely used. Programs like PECS and PROMPT therapy are also effective. To know which option best suits your child, you can reach out to our training center for professional guidance.
Will my autistic son ever talk if he hasn’t started by age 4?
Many children show speech growth after age 4, but others may remain minimally verbal. Progress often depends on early intervention, consistency, and tailoring therapy to your child’s strengths. If you’re unsure, it’s a good time to contact our training center for a personalized assessment.
At what age do autistic children start talking in complete sentences?
Some may form simple sentences around 3–5 years, while others take longer. Many autistic children first echo words or use short phrases before building into fluent sentences. With practice and therapy, even delayed speakers can gain meaningful communication skills.